Okay, my audiogram has been posted. Hopefully that will narrow down the advice given for my situation.
Also, I showed the audiologist suggestions presented by @Neville and @Alex_D1 in terms of matching the 2017 Oticons I like, as well as trying out generic fitting formulas, on the new Oticon Owns.
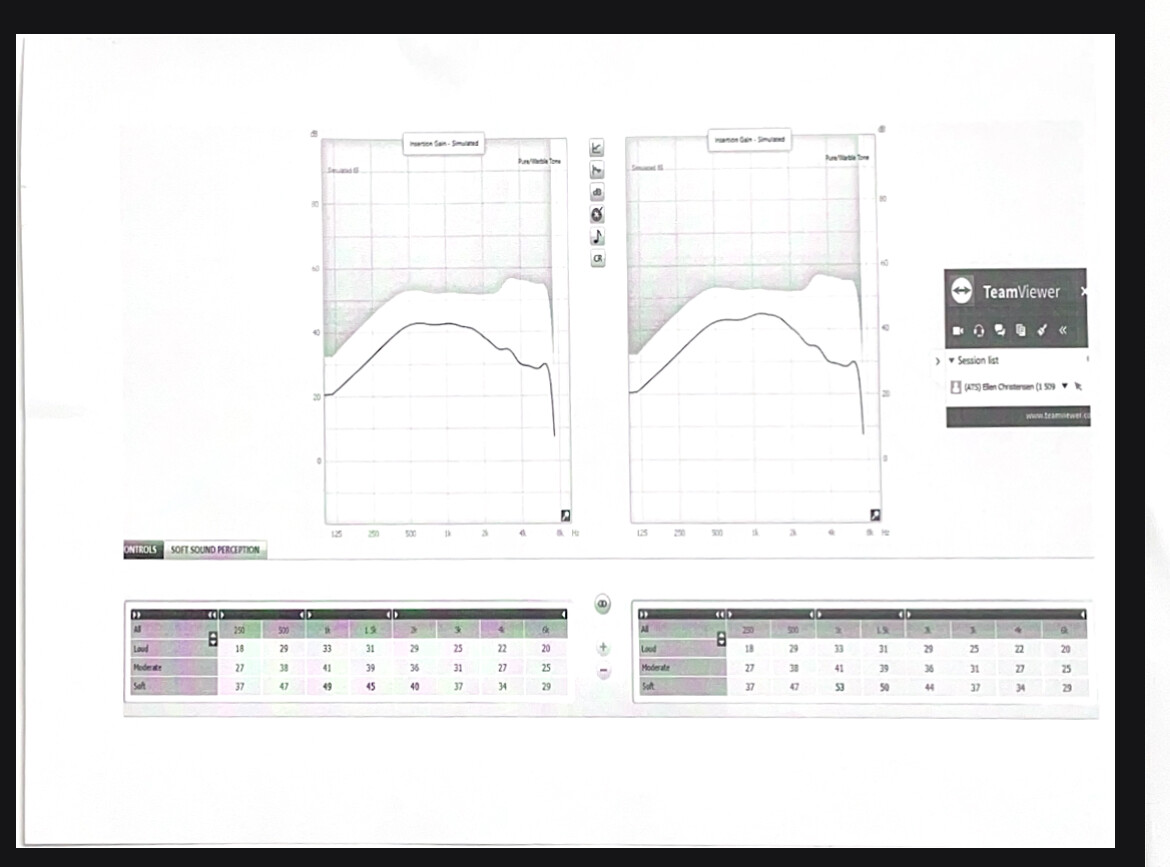
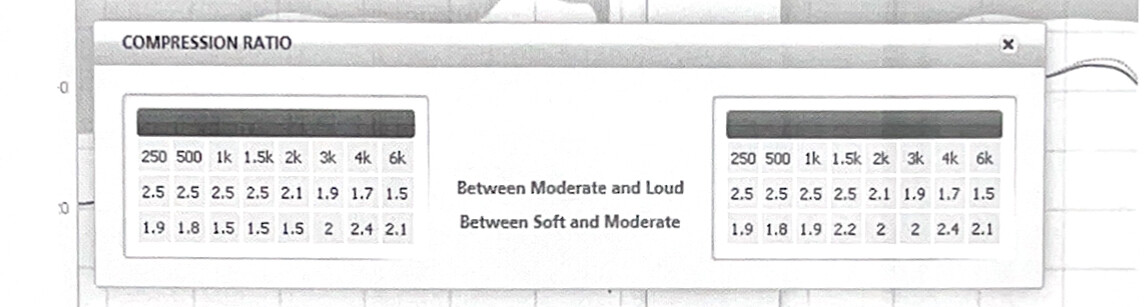
I have included screenshots of the 2017 Oticon gain charts along with their compression ratios, for reference. By the way, these are Nera2 Pros, as I found out today.
The audiologist was open trying the suggestions. She got an Oticon support person on the line who is the one who actually did the matching via screenshare.
Matching the MPO and gains didn’t seem to do much, especially since the MPO was already apparently maxed out on the new Oticon Owns. Neither did changing the Owns to generic, linear, and “pediatric” fitting formulas. When the latter was tried, the compression ratio was 1:1 across the board, so very little compression. But none of these solved the issue, the sound was still too soft, “tinny”, and the bass missing.
Then the compressions were matched, and suddenly the volume was much higher, to a point that there was a tremendous amount of feedback (the feedback analyzer was afterwards run to eliminate it). It sounded much closer to my 2017 Oticons, with the exception of the bass, which, while better, was still largely absent.
Which was all very surprising, apparently. Both the Oticon technician and the audiologist were at a loss on how this occurred, because the compression ratios on the 2017 Oticons range 1.5-2.5, HIGHER than the Owns. They said that increasing the compression on the new Owns to match it should SOFTEN the sound, not raise it.
Why did increasing the compression ratio drastically increase the volume/power?
At any rate, I still wasn’t pleased with the lack of bass, so I returned them. I will wait for further help here before deciding what model/make to try next.
The 2017 Oticon Nera2 Pros:
 Good Luck with your journey I hope you’re able to find a devices that you are comfortable and content with.
Good Luck with your journey I hope you’re able to find a devices that you are comfortable and content with.