My 6 yr old was recently diagnosed with conductive hearing loss in his left ear only. After several audiograms and tests, we are now moving forward with a hearing aid.
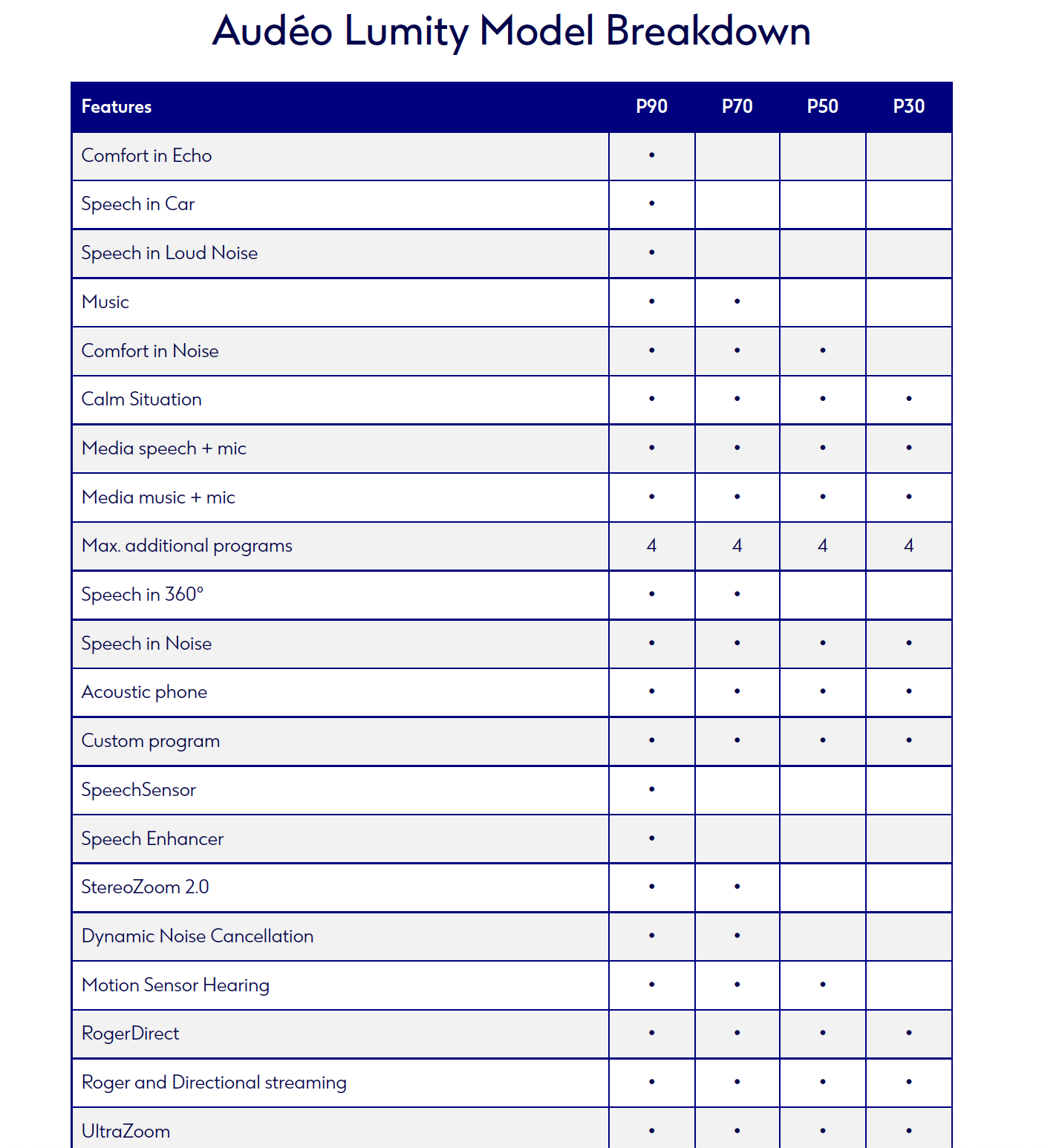
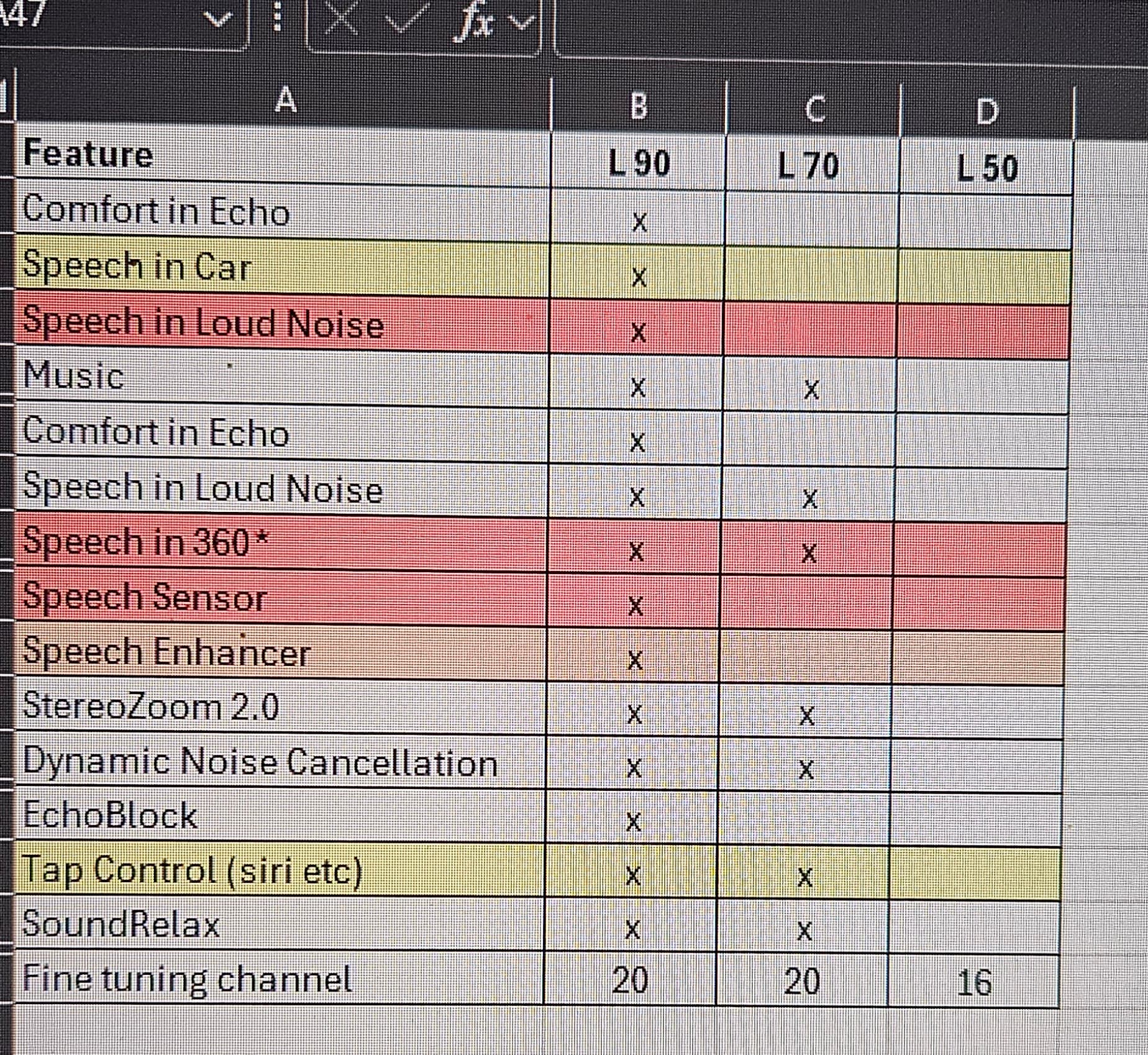
Our options are the Phonak Lumity L50, L70, or L90. I’ve been reading that many of the L90 additional features require 2 hearing aids to function. I found this breakdown of the features but am having a hard time understanding which features are useful/needed/work with one 1 HA and which ones he (as a 6yr old with no tablet or phone of his own) doesn’t need.
Our insurance isn’t covering it so we want to be price conscious while still getting him the best one for him.
You’re showing information for the Audeo Paradise model, but he’ll be getting the Sky Lumity BTE, right? And he’s with a pediatric audiologist?
The 90 is probably overkill for him. The 50 and the 70 are both fine, I might lean towards the 50. Consider that this will probably be his hearing aid until he is 11 or 12 and then he will likely need a new one. (That’s closer to the age when some children transition from BTEs to RICs if they want to.)
L70 have the option for Speech in Loud Noise, but only for a separate programm, which have to be setup by the fitter, and you need to activate this programm manually.
L90 does have Speech in Loud Noise as a automatic program in Autosense . And you could also set/add it as manual program.
Note: for the following functions two hearing aids are needed:
I’m not sure about “SpeechSensor” and “Speech Enhancer”
In this video for SpeechSensor there is no indication about the need for a binaural pair of hearing aids.
“Speech Enhancer” is for soft speech in quiet environment (a special feature for Programm Calm Situation )
Hi Jessie. I have no pediatric hearing aid (HA) exp. but suggest to be cost effective a few ideas/comments:
The audiologist you are working with should provide you both with the cost breakdown for the different tech levels AND how your child might benefit from each increase in tech level, as well as their recommendation. @Neville is very experienced and I’d take his comment that L90 is overkill - unlike your audi, who has a potential conflict of interest (selling you more than what is cost effective).
If this audi works well for you, you will have a multi year relationship so I’d perhaps request:
For adult HAs and I assume true for SKY Lumity an audi has a demo model which allows them to set it up as L50, L70, or L90 (I believe such change can simply be done remotely). Thus discuss having your child 1st try things (2-3 weeks) with L50 level of tech, and then now that she/he is used to the sound of HA then have it changed to L70.
By asking your child ?s and observing them you might be able to decide e.g. the L70 is supposed to (on paper) be better in X or Y situation, BUT I don’t observe it being any easier for my child; or if any benefit is there it is not obvious.
And if there is benefit then be able to assess is the benefit worth the additional $___ cost; or would that money be better spent on other kinds of listening support for my child.
My son who just turned 40 had very severe dyslexia so I have some exp. with making cost effective decisions for supporting one who we love dearly, and as you are experiencing and navigating it can be overwhelming as we want what is best for them. My son’s 1st private professional tutor/coach shared with us/parents that his dyslexia was so severe that they thought that even with compensations that he’d struggle and most likely not be able to make it through college. She just wanted us to have reality based and realistic expectations. She ended up being quite wrong and while it took a great deal of special training my son successfully completed grad school. I hope that my son’s story is encouraging for you and family. Hearing aid technology continues to improve significantly so I hope/predict that things will be far easier for your child quickly.
Finally the HA hardware and technology is probably only 50% or less of the “intervention” the other is the skill and exp. of the audi. Meaning their rapport with your child, their eliciting from child what they are experiencing and hearing, and then with that information adjusting/fitting the HAs to suit your particular child. Initially the HA in the box is like a blouse on the clothes rack, and give it to two different seamtresses to fit it to you and the result will likely be quite different.
Final thought, and perhaps you have already been offered this … if it is possible for audi or other professional to have you put on headphones or some other device and then simulate what it is like for your child to hear, this might be invaluable information. I had such simulation with regard to some aspects ofmy son’s dyslexia which both assisted me in understanding his challenges, but also helped me behave differently when reading out loud with him so that it was a more optimal learning experience.
I hope some of this is helpful and doesn’t add to overwhelm. Good luck to you and your child, and welcome to this forum that has so many helpful and knowledgeable members.
It’s actually a bit odd to me that you’re asking here. Are you 100% sure at this time that your son is with a pediatric audiologist. That’s the most important thing. What’s currently being done to look into the etiology of your son’s hearing loss? I don’t really need to know as long as the answer isn’t “nothing”.
Children are different than adults and it’s not really a process of tweaking the hearing aids to their tastes, it’s a process of accurately hitting prescriptive targets and applying evidence-based practice and then coaching you on supporting continued wear. My expectation when a child comes to me from another pediatric provider is that the settings in the hearing aid will be 98% identical to how I would also fit them, which is following some pretty rigid guidelines.
The speech in loud noise program should not even be an option for your child, nor should any of those directional programs that pop-up in the higher tech options. Children do not reliably turn their heads towards a speaker, so apart from some basic pinna effect filters most directionality is simply turned off for children and doesn’t start to get turned back on until kids are older. Even then, I think most pediatric audiologists would be pretty conservative about accessing narrow directionality until well into adolescence.
The 70 level provides a bit more flexibility for the clinician in the event that noise complaints have to be managed and slightly better ease of shaping the frequency response, but if there are no noise complaints much of that noise reduction may also be left off for a long time. They also offer a bit more room to “grow into” in terms of features that may be turned on over time if your child keeps them functional long enough.
Did the audiologist not guide you towards a certain level? With their reasoning explained? Maybe they did and you didn’t mention it, but it’s the lack of that that makes me wonder about whether you are seeing someone who usually sees children.
And on the outside chance that your son is actually being seen by a hearing instrument specialist–>absolutely not. I love our HISs, but they should not be seeing children without the direct oversight of an audioloigst.
So he has conductive hearing loss due to a bone spur on his stapes bone. Yes, i am confident both his ENT and Audiologists are familiar with peds as he is seen in the pediatric ENT/Audiology department at Mayo.
I did ask her for her opinion (after i posted this a.m.) and she recommended the 70. She agreed that the 90 is overkill. She did say, given his medical history/results that she thinks the noise cancelling features (probably not the right name for it) will be beneficial for him.
We do get to try it for 2 months and then can return it if its not the right choice.