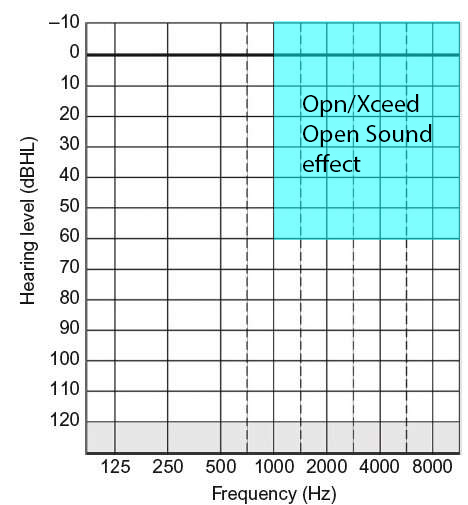
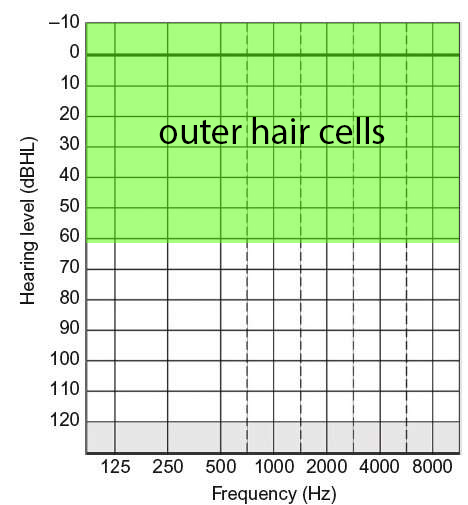
Hello all! I want to warn about Oticon Open Sound efficiency for specific hearing loss. As we know, we have two layers of hair cells - inner and outer. Outer hair cells have much higher frequency resolution and sensitivity than inner hair cells. It’s an upper half of audiogram blank. In addition, we have the ability to determine the direction of sound at high frequencies. It’s a right half of audiogram blank. So the best information about sound localisation placed in upper right quarter of audiogram blank. So if your audiogram line does not cross this quarter from left side to right, you will lose spatial sound information, and Opn/Xceed will sound as cacophony for you. I think Oticon knows about this, but hides it for sales growth.(upload://uRYKmBJzJJZjzsGHGDC82XHHDKK.jpeg)
![outer cells|463x500]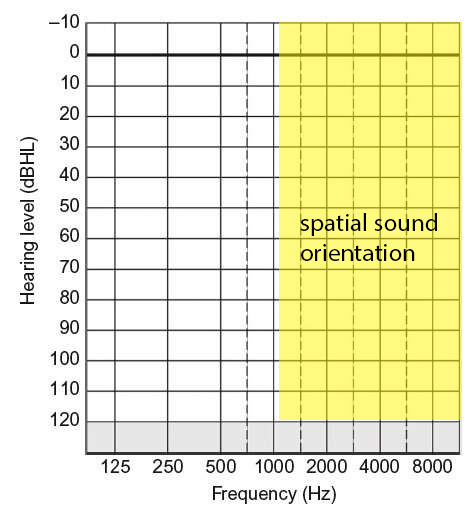
Following. Want to see more info on this.
I think what you are saying is that we need higher frequency sounds for good directionality. Low frequency sounds sound like they are coming from everywhere, and have little directionality. That is why we can get away with using one subwoofer in a sound system, and it does not matter much where it is located. We get directional sense from the time delay to the further ear compared to the nearer ear. This is aided by our head being in the way.
I would agree with that, but would suggest that is a problem for all hearing aids, not just Oticon. Directionality will suffer with uncorrected high frequency loss. And I really think “open sound” is just a marketing term to get attention, and not a distinct characteristic of the aids.
Hearing aids can only do so much to help with hearing loss like you have. My loss is no where as bad as yours and I find as my hearing loss becomes worse that hearing aids become less able to help. I have OPN1 ITE hearing aids at this time so I do not have the open sound. I have done my research due to getting new aids this summer, and I have found that from that research and reading a lot of reviews that the open sound only seems to help the ones with mild to moderately severe hearing loss. In other ones the ones that can wear the open domes. I sure can’t wear open domes any more so I do not see OPNS aids doing any better than the OPN1 aids that I am know wearing.
CVkemp - I hope OPN1 ITE aids are workin out well for you. Though I’m too lazy to look up fitting chart for your aids, I wonder if your hearing loss fits well within the OPN1 ITE adjustment limits? I see where Oticon has a OPN ITC (canal aid) and assume you are using the same but calling it a ITE (ear aid). Just curious if such a small canal aid is really providing the power/gain you hearing loss requires.
My hearing loss runs from moderate in the low frequency to severe in the mid range frequencies to moderately severe in the high frequencies, My aids fit great if I was content with a REM comfortable fit, but I want my aids set so I can understand speech at any time so my aids are being pushed to the very limits and right on the edge of feedback. I will be getting new aids this summer and I am doing my research at this time. Now my aids could be remaded to have smaller vents, and maybe if needed, which I am not sure they need them, larger recievers. So yes ITE hearing aids will fit hearing loss right on the line of being profound.
OK, I got confused on your time line. I thought you possibly purchased new aids last summer, when you meant this coming summer you plan to buy new aids. I do think you are pushing things if you want your current HA’s remade with smaller vents and/or larger receivers. Personally I wound never “remake” a hearing aid that was being pushed to its very limit unless no other option. Reason being when a HA is pushed to its limits you risk feedback and sound distortion. Secondly any reputable Audi would tell you up front, you have very limited adjustment range to play with if you happen to have a decline in hearing.
But if you do trial new aids this summer I personally would recommend half shell to full shell or possibly behind the ear, versus a ITE or ITC aid. You want a HA to last five plus years and not forced to rebuy sooner due to exceeding hearing loss range of what ever aid you buy.
I get my aids from the VA, and at my annual hearing test, my Audi informed me that he was getting me new aids this summer and for me to do my research and look at what is coming out this spring. I was surprised seeing normally with the VA I would get aids every 3 - 5 years depending on a lot of things one being changes in hearing loss. The VA by default practice prescribes hearing aids for the user to be comfortable, which really means for me that my speech understand sucks. I want my aids set up for max speech understanding. My Audi was new to me when I first had my appointment at the clinic I now use. Over the year plus I have known him he has come to know me extremely well and he now understands my needs and desires. I see my next aids as being somewhat uncomfortable at first, but I know I will be able to adapt to them.
Yes I am different than most on here. And with the help of my Audi and my desire to research I have learned a lot this last year and my Audi has said that he has learned a lot because I have pushed him to find answers for my questions and my pushing to understand speech so much more than I do.
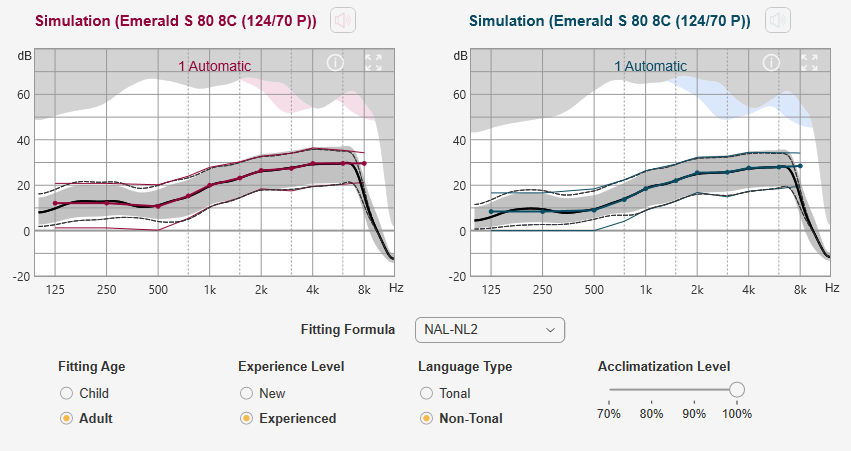
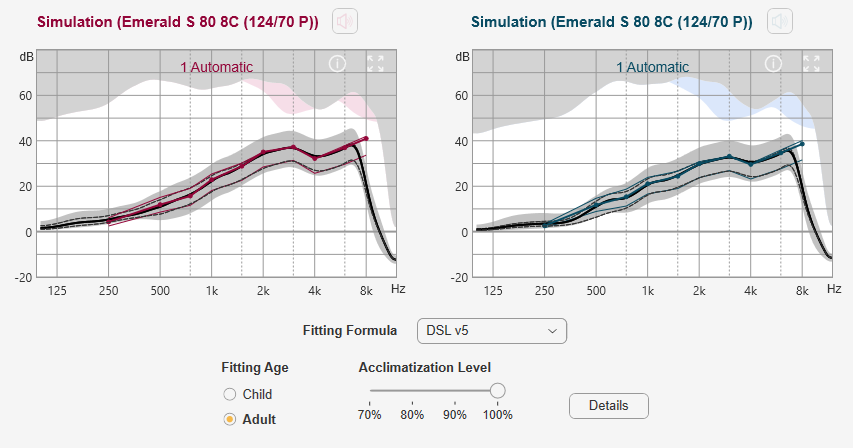
@cvkemp, I know I have made some suggestions before, and at the risk of contradicting what I said before, my suggestion would be to go with a RIC style using a P power receiver. The RIC style has more protection from feedback, and better directionality due to the location of the microphones.The most critical parts would be getting the right fitting type, and the fitting formula right. I believe you have a custom mold CIC type now, and must know whether or not you can tolerate a custom mold in the ear. Assuming you can I would go with a custom mold on the RIC style as well to get the most gain and most protection from feedback. Here is what an RIC type with custom molds (1mm vent in right, 1.6 mm in left) would look like with the NAL-NL2 formula. You would have lots of room for power and feedback avoidance.
The other option is DSL v5. It has much less compression and lower gain in the low frequencies. This should result in less annoyance from background noise, while still having good speech recognition. But, that is simply a guess. The best way is to try both formulas and see which one you like. Then move on to fine tuning the best one. I’m sure however, they will sound different. Regardless of which one you pick, I think a RIC style would be a significant step up. The brand does not matter so much, as long as it works with your choice of phone.
I have the larges half shell you can have and not be called full shell ITE aids. I may go to Rite aids but I am very much against them seeing, I wear glasses and when I go outside I have to have full wrap around sunglasses that fit over my glasses due to my eye conditions. That doesn’t leave any room for BTE hearing aids. And I even get my glasses from the VA so they know and understand my issues.
I have done a lot of research on molds (and in the end could not tolerate them). My conclusion is that the feedback suppression comes from the portion that is in the ear canal, not the part that is in the outer ear. Some believe incorrectly that the outer shell part helps control feedback, but it does not (according to good studies). The outer part is only needed for retention of the mold. In the CIC style it of course is needed to house all the electronics and receiver too. I think the best style of mold is the simple canal only (#12 at this link), if they will stay put in your ears. It comes down to your specific ear canal shape. As for material there seems to be some evidence that a silicone might be better than acrylic, but some dispute that. The canal type is also the least visible. If it will not stay in, I would go to the canal lock (#4) next. It adds a little bit of extra retention.
I wear glasses and don’t find them to be much of a problem at all with the RIC style. Yes, there is the occasional click when the aids hit the legs of the glasses, but not really a big issue. Keep in mind that smaller is better. Replaceable battery aids tend to be smaller than rechargeable ones, and fit better behind the ears, although that could vary a bit from brand to brand. A 312 is probably big enough for your loss, without going to the extra bulk of a 13.
the larger shell houses the electronics for my fully connected aids, what is in the canal is only the receiver and the little extra for the vent. And yes if I did not need the over glasses wrap around sun glasses the BTE aids would work. And to be honest if I end up with BTE aids it will because I go to aids that have t-coils and are rechargeable, which means they will be a little larger. If there is one thing I miss, it is the t-coils.
Perhaps some prescription eyeglasses that are intended for those with fuchs dystrophy, instead of wearing two pairs of glasses?
As someone that has had all ITE hearing aids, and I have worn Minirite aids for about 3 years and did not like them for many reasons. But mostly they are not good for someone that rides motorcycle or Vespa Scooter like I do. BTE hearing aids sucks for wearing motorcycle helmets. Also I am a hiker and again the BTE aids get swept off by tree limbs.
But most of all I just do not feel comfortable with BTE aids, and I do not think that the sound of BTE aids even come close to a well fit ITE hearing aids.
Agree with the motorcycle helmet issue. It is near impossible for me to wear RIC aids with a full face helmet. I just take them out. I don’t think your loss is sufficient to consider BTE aids. RIC P power should be enough.
I wear BTE’s and ride with an ARAI 3/4 helmet. Fits greats. I’m anxious for the these bluetooth aids to be able to connect to the motorcycle with the right adapter.
Ehhhhh, this (the original post) is simplified to the point of being kind of wrong. Only inner hair cells send information about what you are hearing to the brain. Outer hair cells functionally change the response of the basilar membrane in a way that makes inner hair cell activation more sensitive and specific. So you are correct that when you lose outer hair cells, you lose sensitivity and resolution. There is a rule of thumb floating around that any hearing losses below about 65 dB are largely outer hair cell losses. This is generally true but not necessarily/completely true. Even people with more moderate hearing loss can have inner hair cell loss, or supporting cell loss.
To localize sound, we use the time differences between when a sound hits one ear versus the other, the level difference between when sound hits one ear versus the other, and the different spectral filters that result from sound hitting the pinna from different angles. Time differences are useful roughly below 750 Hz, level differences are useful roughly above 3000 Hz, and pinna filtering is useful roughly above 6000 Hz. ALL of these are difficult with hearing loss and hearing aids. Hearing aids don’t really try to address time differences, they just assume that the hearing aids will process things at approximately the same speed and so time differences will magically fall out right. However, I think this is probably arguable. The normally functioning human auditory system can detect 10 microsecond differences. Is there an engineer on here who can speak to jitter/lag in electronics? Some manufacturers try to process things in a way that will maintain level differences, but if you have significant hearing loss at 3 kHz the benefit may be limited. For many people with hearing loss, pinna effects are right out. (For anyone who is interested, we can detect 1-2 dB level differences, and yeah we are worse at localizing sounds in that gap from 750-3000–good thing most sounds in nature are broadband.)
So, that’s the biology.
The idea behind Oticon’s Opn strategy doesn’t actually have much to do with improving your ability to localize sound, so all of this localization talk is a little bit beside the point (although off the top of my head I do think Oticon is one of the manufacturers who tries to maintain appropriate level differences). The Opn strategy, put simply, reduces background babble without the use of narrow directionality, which is why they called it “open”. It DOES do this, and it’s cool. However, it can only do this in a fairly moderate way. They claim a 9 dB signal-to-noise improvement but I would be pretty skeptical as to whether that translates out of the lab and into real life, and for which users. For someone with your level of hearing loss, 9 dB is absolutely insufficient for you to benefit in the sorts of difficult listening situations that Oticon advertizes.
DSL v5 is normally associated the children’s prescription.
So I found the results of these studies with adults and elderly interesting:
https://www.tandfonline.com/doi/full/10.1080/14992027.2019.1697902?af=R&
I think my fitter was a bit surprised when I asked to try DSL v5. It seems the industry is somewhat misinformed about it. The usual assumption is that it is for children only and it is quite new and untested. The fact is there is an adult and child version of it, and has been around for quite a few years even in the v5 version. She even commented to me that she was unaware that it was available in their fitting software, and that I was the first customer that she ever used it with.
Not sure about private practices, but I get the strong feeling that Costco depends heavily on their suppliers for support and training. And, I’m sure each hearing aid supplier lobby them pretty hard to use the manufacturer proprietary fitting formula for their aids.