Starting a new thread so as to keep this one on topic. Testing for magnesium deficiency is easy and often done in people with arrhytmia problems including atrial fibrillation. If one is inclined to want to take supplements, I’d encourage that one consult with one’s physician. Taking extra magnesium can be dangerous for those with poor kidney function.
Strangely enough @MDB, I just ordered some Magnesium Taurate from Amazon a few hours ago, along with some Iron Supplements, and Vitamin C… Currently suffering from Chronic Fatigue, that seems to be getting progressively worse, I use proscribed Beta Blockers, for anxiety & wild fluctuations in my heart rate, I also have type 2 diabetes… I am hoping for a slight improvement in my constant tiredness, I have had several blood tests over the last couple of years, from my GP, but nothing seems to show up… I thought, it might be Iron Deficiency, (I don’t eat meat) after my daughter suggested as much, she is a staff nurse, with a master’s in nursing, along with a couple of other degrees… I will try to incorporate these supplements gradually, and hopefully see some improvement? Cheers Kev
Well @MDB…This proverbial car, is running on fumes at present Constantly falling asleep at the drop of a hat, it is fastly becoming a major issue, even when I get a good nights sleep, I’m still tired…Perhaps, I’m clutching at straws, but the medical profession don’t seem to know, apparently its not a thyroid problem… Our 2 local doctors surgeries, are a disaster area, we have no resident doctors, so there is no continuity of service, we only see locum’s, well that’s not true, we only get telephone appointments with locum’s… NHS Highland took the service away from the local doctors, because of the inundation of serious complaints about the lack of service, or to be be more specific, the service was so understaffed, it wasn’t fit for purpose (recruitment issues in a remote area) those doctors whom remained, took umbrage at NHS Highland taking over the service, and left en masse… So at present, if you are “ill” in my area, you don’t have many options, and self medication seems the only logical conclusion? The local doctors service has gone beyond abysmal, in truth, it takes approximately 2 weeks to get a telephone consultation, and yes, you could be dead by the time you wait! There is plenty of good doctors surgeries in the Highlands, unfortunately if you are not registered their, they can’t see you! I am sure it will eventually be sorted, but that’s perhaps another 2 years down the line… Cheers Kev
Oh gosh Kev it sounds like a rough patch, to put it mildly.
I HAD afib until I got an ablation; I still have sleep apnea and treat it every night with a cpap machine. I LOVE my cpap machine. It’s allowed me to finally sleep through the night and dream. And I feel rested in the morning and not grouchy and angry from lack of REM sleep. Apnea sufferers most often don’t know how bad it is because they’re always half asleep, desperately trying to sleep and also desperately trying to breath. It’s a never ending battle without a cpap machine.
Potassium and magnesium are necessary for heart health for sure. There’s a great site called StopAfib that has good discussion by folks who’ve suffered from afib, or are suffering still and have questions. It’s NOT a piece of crap whoo-whoo non science based site.
Having poor medical care is more than frustrating and you’re obviously free to do as you choose. I just don’t think it’s wise to start adding things without knowing if your body needs them or not. There are simple tests that would tell you if you’re deficient in iron or magnesium. It’s likely the doctor already checked your blood count (which would tell if you’re anemic which would be the case if you’re low on iron) if you complained of tiredness (I assume that’s why they checked thyroid?)
As @jeffrey suggested, sleep apnea is a real possibility based on your symptoms. Best of luck.
I recently had a mini stroke, and before that, was called in due to dangerously low Pottasium (from a riutine blood test). Also type 2 diabetic. Hyper Tension is my biggest worry. I just collected my monthly batch of tablets… I should have taken a trolley
I also have sleep Apnoea, but (probably) due to a misaligned septum, I can’t live with the machine.
Thank you @MDB & @jeffrey, I was checked years ago in the sleep clinic for Apnea, but they said I was fine… Although, my wife Elspeth has it, she uses the breathing machine every night, usually blowing down the back of my neck In truth, I probably won’t find a suitable solution, with or without medical intervention, in most instances they guess, sometimes correctly, and sometimes not… It is what it is. If I try anything, I will be cautious…Cheers Kev
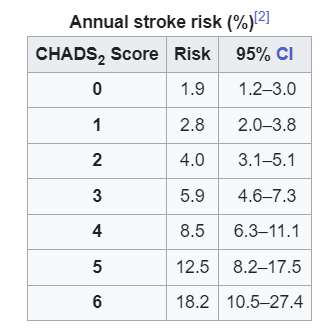
I have been diagnosed as having paroxysmal atrial fibrillation - rare episodes that defy monitoring. A WebMD article that I can’t find now said that rare episodes are usually the first way Afib appears in aging folks but, unfortunately, the Afib episodes then typically become more and more frequent. Magnesium levels have not once come up in discussions of how to improve my situation. Avoiding alcohol, hydration, adequate sleep, avoiding anxiety, potassium levels, TSH levels, weight mgmt (no problema there), exercise, etc., have all been discussed. I’ve only had two really noticeable episodes in two years. The latter one caused my electronic heart rate to go over 160 bpm (as high as 258 at one point) but caused my blood pressure to drop dramatically to 60/40 with a BPM-recorded heart rate around 70 - indicating most of the electronic beats were ineffectual fluttering. My cardiologist said on the basis of the 2-hr duration and severity of that episode alone and my age, I should be on a strong direct anti-coagulant. On the basis of the CHA2DS2–VASc score - Wikipedia, I should be, too. I have had a number of blood tests for electrolyte balance, etc., and I score within an acceptable range for all of those. I’m now taking Eliquis 2x daily.
So, a principal risk of Afib is throwing a clot to the brain. Do worry about electrolyte levels, but finding out whether you should be on a modern anti-coagulant might be the most helpful.
The most impressive part of the Wikipedia article that I cite is the annual stroke risk based on your CHA2DS2-VASc score.
My primary care physician wanted me to start taking a beta-blocker, but I didn’t want to possibly reduce my heart’s ability to respond to exertion. My cardiologist and my PCP were OK with me just carrying tablets of metoprolol around. The PCP warned that in an emergency, the drug might not take effect for 30 min. The cardiologist advised if needed to chew a tablet to speed the blocking reaction, contrary to normal usage instructions: “Do not chew!”
I still can’t find the article I read that said age-related Afib usually starts in older folks with sporadic events that become more frequent, but WebMD has a great, EXTREMELY detailed guide to Afib.
Here’s a link to an article on OTC supplements for Afib. Magnesium is mentioned first, but as MDB says, there’s a proper balance, and testing is advisable.
Your description of how afib often starts certainly fits my Mom’s history. Hers started when she was about 80? Initially controlled with cardioversion and medication. Gradually became more frequent until she was in it most of the time. She was on warfarin (early anticoagulant) for years. She eventually died from stroke at 93, but it was from vascular disease, not from throwing a clot from her heart.
In my experience my heart will respond to exertion even with a beta blocker holding down the rate. It’s as if the drug and the body’s signals are in a “tug of war”.
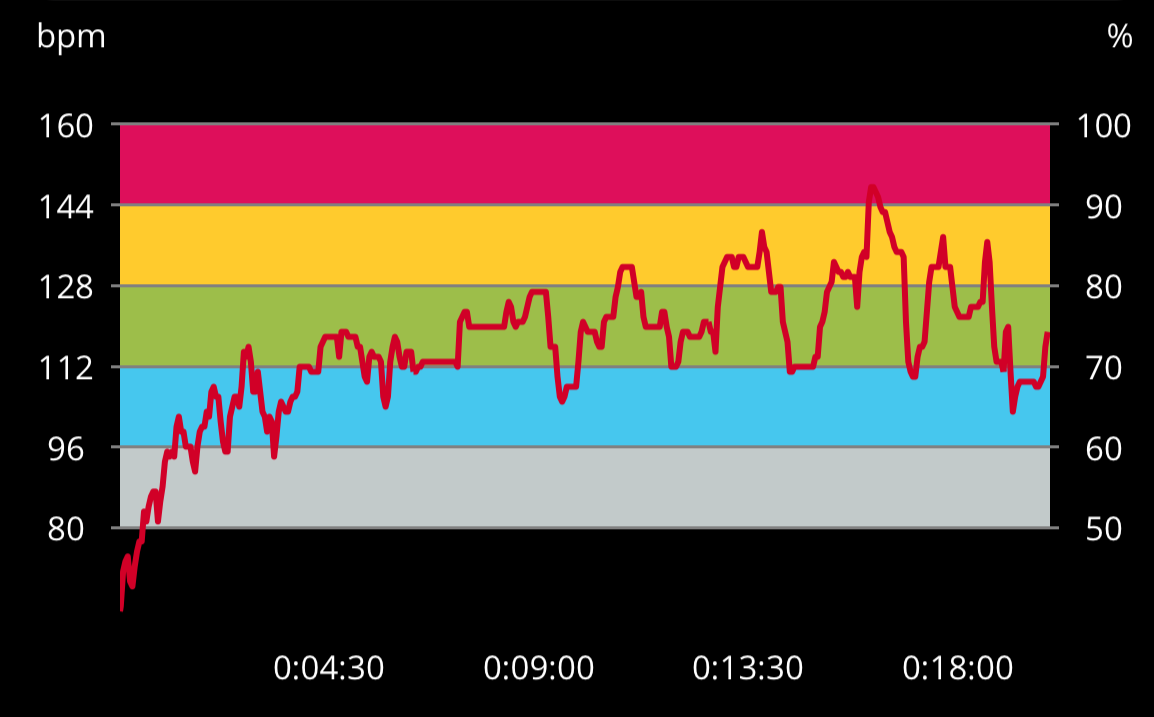
I’m in afib all of the time and take metoprolol at a dosage that brings my resting ventricular rate down to the 60’s or lower. Here’s what my Polar monitor showed during one treadmill session:
@x475aws. Perhaps it’s just me perusing web info on possible side effects of metoprolol, but some of the possible side effects are fatigue, drowsiness, etc., which is also part of what scares me off, too. Most of the time, my heart rate is fairly normal (72 bpm right now after a light cup (1/3 tsp) of Folger’s freeze-dried coffee). I had left exercise out of my doctor-recommended lifestyle list for dealing with Afib, but I’ll add it to that prev. post now. But I think I’ll wait to see if I get into all-the-time Afib before taking a beta-blocker. My PCP is keen on trying ablation - but that seems silly if 99.9% of the time I have nothing to monitor.
Sorry to say that Afib tends to be progressive about 97% of the time. People look for lifestyle changes and triggers to stop it, but…it usually becomes more and more frequent and severe over years. No matter what. Early intervention through drugs or an ablation has the best chance of success. You don’t want this condition to develop! It’s horrible.
It’s not about your heart muscles or valves or blocked arteries or anything like that. It’s about the electrical impulses controlling your heart rhythms. Olympic athletes get afib. You can’t muscle your way out of in any more than you muscle or diet your way out of your poor eyesight. So think of it like that.
And by the way, yes afib can cause strokes. You REALLY don’t want that. I suggest being aggressive as this condition first rears its ugly head.
I think it’s similar to the fact that a good body weight can’t keep you from dying. However, controlling your body weight can help prolong your life and help control various medical conditions. Whatever propensity you have to have Afib, controlling various factors can help minimize the chances of having an attack. You’re more prone to Afib attacks if you drink heavily and gulp your booze down in a few swigs, if you’re dehydrated, if your potassium levels are low, if you’re very sleep-deprived, etc. My wife is a board-certified internist who, by her practice, is essentially a geriatrician. She said when I asked her just now that control of lifestyle factors can moderate the propensity of your heart to engage in episodes of atrial fibrillation. Just do an Internet search, for example, on whether alcoholics are more prone to suffer atrial fibrillation. That’s a lifestyle factor that damages your heart… I only drank in moderation (45 ml of 80-proof vodka a day), but both an RN practitioner and my cardiologist advised me to give up drinking, saying alcohol is a cardiac poison. So I did.
I imagine your doctor wants you to do something because of the ventricular response to your 2nd noted AFib episode. It isn’t so far from there to dying. Or getting in the paper as a driver who lost control because of a medical condition.
Metoprolol is a very benign drug. You might have no trouble with it, or any side effects might go away as you adapt. If it doesn’t work out, stop taking it and it’s gone. And it’s cardio-selective, so doesn’t mess up sexual function like non-selective beta blockers.
Although I think it’s generally better to follow doctor’s advice, I don’t think Jim’s choice is particularly unwise. It’s quite possible that the dose of metoprolol that Jim would tolerate when he was in sinus rhythm wouldn’t be enough to keep him out of atrial fibrillation or keep his rate low enough if he did go into atrial fibrillation. My Mom ended up needing a pacemaker to tolerate an adequate dose of metoprolol. Her rate in atrial fibrillation was fine but if she would convert to sinus her rate would drop into the 30’s and she’d be lightheaded. A pacemaker was a good fix, but since Jim is basically fine more than 99% of the time, not taking metoprolol seems like a reasonable decision. Ablation can be useful, but in my opinion has been oversold. It often doesn’t last and people still end up on medication.

 Constantly falling asleep at the drop of a hat, it is fastly becoming a major issue, even when I get a good nights sleep, I’m still tired…Perhaps, I’m clutching at straws, but the medical profession don’t seem to know, apparently its not a thyroid problem… Our 2 local doctors surgeries, are a disaster area, we have no resident doctors, so there is no continuity of service, we only see locum’s, well that’s not true, we only get telephone appointments with locum’s… NHS Highland took the service away from the local doctors, because of the inundation of serious complaints about the lack of service, or to be be more specific, the service was so understaffed, it wasn’t fit for purpose (recruitment issues in a remote area) those doctors whom remained, took umbrage at NHS Highland taking over the service, and left en masse… So at present, if you are “ill” in my area, you don’t have many options, and self medication seems the only logical conclusion? The local doctors service has gone beyond abysmal, in truth, it takes approximately 2 weeks to get a telephone consultation, and yes, you could be dead by the time you wait! There is plenty of good doctors surgeries in the Highlands, unfortunately if you are not registered their, they can’t see you! I am sure it will eventually be sorted, but that’s perhaps another 2 years down the line… Cheers Kev
Constantly falling asleep at the drop of a hat, it is fastly becoming a major issue, even when I get a good nights sleep, I’m still tired…Perhaps, I’m clutching at straws, but the medical profession don’t seem to know, apparently its not a thyroid problem… Our 2 local doctors surgeries, are a disaster area, we have no resident doctors, so there is no continuity of service, we only see locum’s, well that’s not true, we only get telephone appointments with locum’s… NHS Highland took the service away from the local doctors, because of the inundation of serious complaints about the lack of service, or to be be more specific, the service was so understaffed, it wasn’t fit for purpose (recruitment issues in a remote area) those doctors whom remained, took umbrage at NHS Highland taking over the service, and left en masse… So at present, if you are “ill” in my area, you don’t have many options, and self medication seems the only logical conclusion? The local doctors service has gone beyond abysmal, in truth, it takes approximately 2 weeks to get a telephone consultation, and yes, you could be dead by the time you wait! There is plenty of good doctors surgeries in the Highlands, unfortunately if you are not registered their, they can’t see you! I am sure it will eventually be sorted, but that’s perhaps another 2 years down the line… Cheers Kev 

 In truth, I probably won’t find a suitable solution, with or without medical intervention, in most instances they guess, sometimes correctly, and sometimes not… It is what it is. If I try anything, I will be cautious…Cheers Kev
In truth, I probably won’t find a suitable solution, with or without medical intervention, in most instances they guess, sometimes correctly, and sometimes not… It is what it is. If I try anything, I will be cautious…Cheers Kev