I am hoping that one of the many people who are in this community can help. My mother is 100. Over the past years (as her hearing declined) she has tried all of the top of the line hearing aids. She is beyond frustrated as it appears that she cannot hear successfully with any of the hearing aids she has tried. Each of the audiologists or Hearing Aid providers has used her audiogram to fit her, yet the issue is the same each time. She can only hear the person who is standing or sitting next to her, whether it’s in a noisy room or a quiet room. Right now she is using Widex Moment and she can barely hear. I know how sad she is with this state of affairs and am hoping that one of you might have some suggestions. She lives in Massachusetts, close to Boston.
Could you share her audiogram?
It might help us help her.
You could try one of these folks:
Has she seen an ENT lately?
Our friend Bud was 90 years old and profoundly deaf and ill from terminal cancer.
When he went to the hospice for his last days, visits were difficult as conversations required shouting.
Then the hospice loaned him a Bellman & Symfon assistive listening device that he found easy to operate. After that we could have normal level conversations (and the doctors liasing with him were greatly relieved).
These devices are an alternative option to check out for your 100 year old mother.
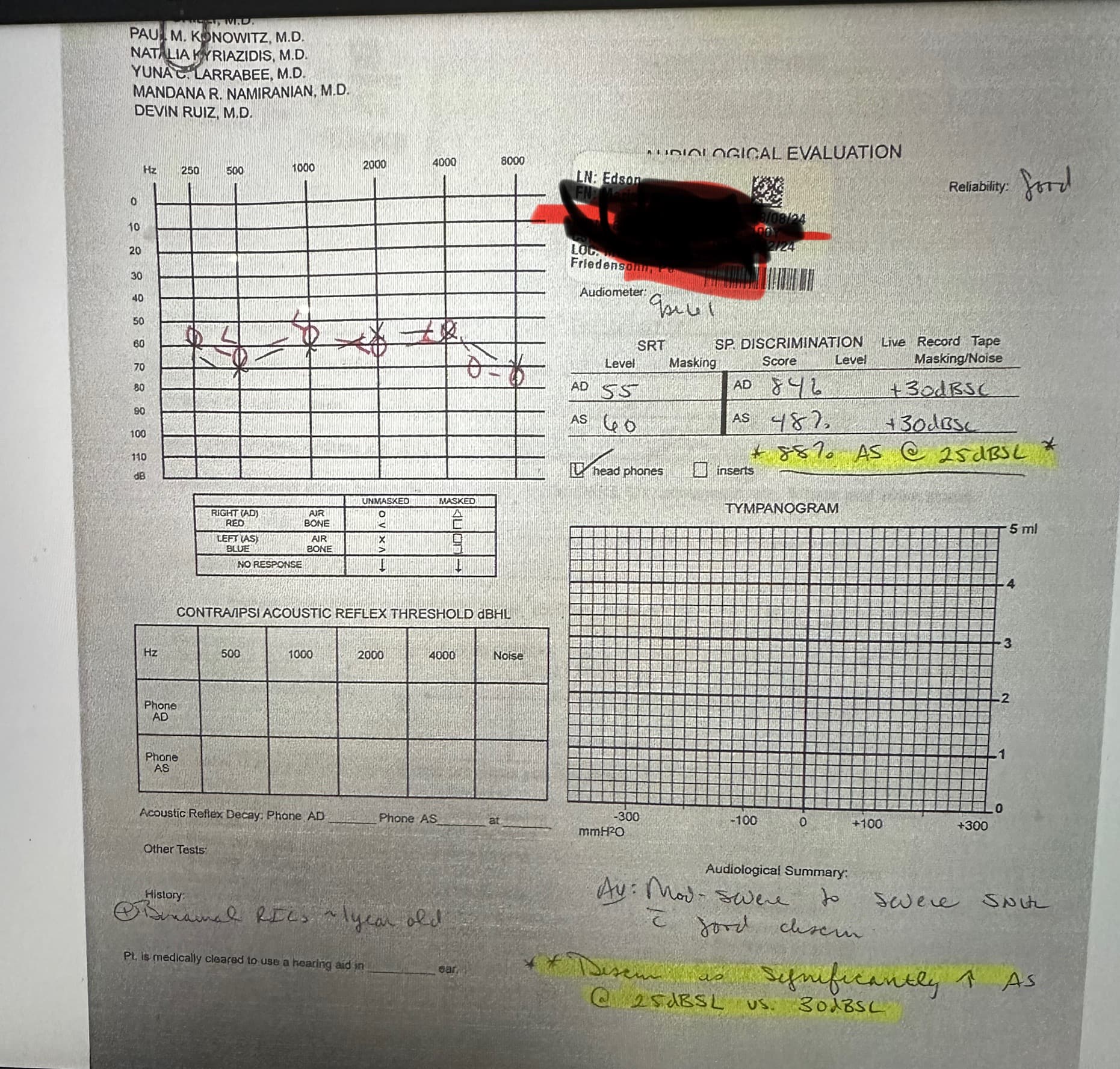
This is my mother’s most recent audiogram. Yes, she has been to more than one ENT, each highly recommended and quite thorough. Each ENT has said that they do not know why she has not successfully found hearing aids that work. One recommended power hearing aids, but none of the hearing aid professionals we’ve talked to thought that was a good idea. She is currently wearing Widex Moment hearing aids and we watched her over Thanksgiving and the hearing aids seemed to block the sounds and conversation, rather than allow her to enjoy being with her family.
Is there another way I can uupload her audiogram? I’m trying with a screenshot and a photo of it.
Yes, she has seen a different one for the past three years—each clears her to get hearing aids, and each says that they do not understand why she can’t get a hearing aid that works for her even with her level of hearing loss. One ENT recommended power hearing aids, but none of the hearing care professionals she’s met with have supported that idea, for reasons I don’t understand. She saw her last ENT several months ago—lovely person at Mass General Hospital in Boston and he was mystified with why this has been so frustrating.
I’ll check it out. Thank you. I see on Amazon that they are selling bone conduction hearing headphones. Maybe that’s an idea, too? I’m so frustrated on my mom’s behalf.
Thanks for the audiogram.
I don’t understand the discrimination difference at 25 and 30 db. Unless the extra 5 db is hurting her causing the big difference in speech understanding.
Maybe one of our pros could help.
@Um_bongo or @Neville
Could be really bad recruitment or distortion issues.
Could be really large or really small residual canal (needs REM).
Could be a basilar membrane/retro-cochlear function that means the system just gets overloaded by amplified sounds. Potentially not enough Auditory centre plasticity to accommodate the changes.
At the end of the day, if you get to a 100 years old with a flat loss, having everything turned up by 1000 times IS going to be difficult to deal with. Plus in your book it’s an ‘everybody else’ problem rather than a ‘you’ problem.
Pick the most basic aid that does the job in a style that the user can manage. Full shell, Genesis 16 ITE possibly with a big VC, fitted with REM at approximately 60% of target - flattened further if there’s any peak weirdness. Two weeks later add 10%, and so on.
It’s a process: it might still not work, but agreed with ALL parties; including the client as to the ‘why’ (preferably) without pushy kids prompting responses, you’d have a chance.
Edit: Have we actually established if she ‘wants’ to hear better?
Thank you for taking the time to explain the possibilities of difficulty.
Thank you for this. Let me answer the last question first. Yes, she absolutely wants to hear and feels devastated that she cannot be part of lectures, discussion groups, dinner table conversation and regular chit chat, all of which she loves! Now, other quuestions to you. I do not understand each of the questions that begin with “Could.” Can I ask you to please expand on each so that I can understand these? As for your everybody else vs. you problem, she knows and accepts that she has the problem and cannot understand why everybody else seems to be getting along better with hearing aids which leads me back to what I wrote at the beginning which is that she is distraught at not being able to hear and desperately wants to hear and feels as if the last years of her life are ruined because she cannot hear. I like your recommendtion about the type of hearing aid, Genesis and assume that this is readily available? I have not heard of this one. Now, as for pushy kids—hardly that. We want the last years of her life to be good and she is willing to buy whatever has been recommended by the hearing care professionals. Two of her “kids” (haha, we are in our 70s) wear hearing aids, two different brands and we are completely fine with following the recommendations of the professionals. You are right, though, they do often seem to gravitate towards the ones that have the most bells and whistles! I’m assuming that a flat loss is not a unicorn and that there are ways of treating this successfully? Again, thank you and I look forward to trying to understand your questions.
Try looking them up on the Internet. That’s how I typically get answers to things I am not sure of or need help with.
You have been given really good information. Sharing this information with her audiologist might help.
Good luck.
I think exactly the same.
So, let me tackle each of these so that I can be clear with her audiologist, who might get prickly since he says he has done all that he can, which is of course, disheartening. MY RESPONSES ARE IN CAPITAL LETTERS TO MAKE IT CLEAR TO YOU. I SO APPRECIATE YOUR INTEREST IN THIS—YOU AND THE WHOLE GROUP OF PEOPLE WHO HAVE RESPONDED. WHILE 100 YEAR OLDS ARE OFTEN IMPAIRED COGNITIVELY AND PHYSICALLY, MY MOM LIVES INDEPENDENTLY IN A CONTINUING CARE COMMUNITY AND IS A WONDER, HONESTLY!
- “Bad recruitment” in the context of hearing aids refers to a situation where a person experiences significant sound distortion or discomfort at relatively low volume levels due to their hearing loss, essentially meaning sounds jump rapidly from barely audible to uncomfortably loud, which is a common symptom of poorly fitted or adjusted hearing aids, often requiring adjustments from an audiologist to address the issue; essentially, the hearing aid is not properly managing the dynamic range of sound levels for the individual’s hearing loss.
Key points about “bad recruitment” in hearing aids:
- Cause:
This phenomenon occurs when the damaged hair cells in the inner ear responsible for hearing amplification are not functioning properly, leading to a rapid increase in perceived loudness even with small increases in sound intensity.
-
Symptoms:
- Sounds suddenly becoming very loud at a seemingly low volume.
- Difficulty finding a comfortable listening level.
- Discomfort or pain when exposed to moderate sounds.
-
What to do: THIS IS WHERE WE KEEP RUNNING INTO PEOPLE WHO DON’T SEEM TO THINK OUTSIDE OF THE BOX! I COMPLETELY AGREE AND THE MORE INFORMATION I GET FROM YOU, THE MORE I CAN BRING IN TO SHOW THE AUDIOLOGIST!
- Consult your audiologist: They can assess your hearing loss and adjust the settings on your hearing aid to better manage the dynamic range, potentially using features like compression or noise reduction to minimize the effect of recruitment.
- Check for proper fit: A poorly fitted hearing aid can contribute to recruitment issues. HOW DO WE KNOW IF IT IS POORLY FITTED?
- Consider a different hearing aid technology: Depending on the severity of your hearing loss, newer hearing aid models with advanced features may be better suited to address recruitment. SHE IS MORE THAN WILLING TO PURCHASE ANY HEARING AID THAT SHE THINKS MIGHT HELP HER! I WILL CERTAINLY TALK ABOUT THE FULL SHELL GENESIS 16 ITE WITH THE BIG VCC, FITTED WITH REM AT APPROXIMATELY 605 OF TARGET.
- Real-ear measurements, also referred to as real-ear verification or hearing aid verification, are an objective measure of what a hearing aid is doing inside the ear canal. A thin probe microphone is placed within 5 mm of the ear drum and a sound stimulus is delivered to the ear via a loudspeaker. Real-ear measurements help to understand the sound pressure level (SPL) provided by the hearing aid and the amplification effect of the ear canal. WHO DOES THAT? I don’t think anyone of the 4 different hearing aid professionals have done that for her over the three years we’ve been trying to get something to work for her.
- basilar membrane/retro-cochlear function that means the system just gets overloaded by amplified sounds. Potentially not enough Auditory centre plasticity to accommodate the changes. IF MY MOM COULD NOT PROCESS LANGUAGE I WOULD AGREE WITH THIS. HOWEVER, SHE CAN EASILY FOLLOW ANY NEWS PROGRAM ON TV WITH THE VOLUME TURNED UP HIGH, AND SHE CAN FOLLOW A COMPLETE AND DETAILED CONVERSATION IN A QUIET ROOM WITH ONLY ONE PERSON NEXT TO HER. AND SHE REMEMBERS JUST ABOUT EVERYTHING THAT HAPPENED OR WAS DISCUSSED. I THINK THAT WAS WHY THE AUDIOLOGIST WHO DID THE LAST AUDIOGRAM REMARKED THAT HER ABILITY TO HEAR WORDS CHANGED WHEN THE VOLUME WAS LOWER, SOMETHING THAT THE HEARING CARE PROFESSIONAL (A PH.D. AUDIOLOGIST DID NOT SEEM TO THINK WAS IMPORTANT.) PRIOR TO THAT, ANYONE WHO SAW HER JUST THREW OUT THAT SHE WAS OLD AND THEREFORE HER PROCESSING WAS IMPAIRED. HOWEVER, I KEPT ASKING THEM IF HER PROCESSING WAS IMPAIRED HOW WAS THAT SHE COULD TELL ANYONE ABOUT ALL THE NEWS SHE’D HEARD ON TV? SO, HOW IS THIS PLASTICITY ASSESSED.
MANY, MANY THANKS TO EACH OF YOU FOR YOUR HELP. I KNOW SO LITTLE AND YOU ARE ALL SO KNOWLEDGEABLE AND I AM SO APPRECIATIVE OF ANYTHING THAT YOU CAN STILL ADD THAT WE CAN USE TO HELP WITH THIS SITUATION. I’M SO AFRAID THAT I’LL SHARE THIS WITH HER AUDIOLOGIST AND HE WILL BE DISMISSIVE.
Early in this thread there were two audiologist recommended in your area. You can bet they use best practices fitting hearing aids.
We see many fitting problems on this forum. Many complaints from members who just didn’t know their fitter/audiologist were not fitting the aids using best practices and getting terrible results and unhappy patients.
If your audiologist is dismissive maybe looking for a better one is in order.
Flat losses are usually easier to fix than ones with lots of transitions or very steep slopes.
Starkey make the Genesis, but there’s 5 other firms that could make a full shell in the ear that would suit. Oticon Own 3 would be fine too. Perhaps a physical hand held remote control might be handy as well.
Work out a strategy (like the 60% +10% +10% etc) that you’re all agreed on with your mum, get the dispenser to lay out the timescale and make sure there’s a ‘what if’ proposition too.
Like I said, it’s a process; and there’s always a risk of overloading the system/making her tired.
Best of luck with her.
There’s very little to add that @Um_bongo hasn’t already mentioned, but I’d reiterate 2 things:
-
the fact that none of her audiologists have performed REMs likely explains a lot of your mother’s poor outcomes. The importance of REMs cannot be overstated. Estimated first-fit settings often significantly deviate from precribed gain levels, especially if your mother’s ear canals are particularly small/large.
-
that degree of hearing loss likely didn’t occur overnight. There arent many interventions I can think of that would likely lead to successful outcomes when left until the age of 100. That’s very late to begin rehabilition. Outcomes would be entirely different if hearing aids were fitted a few decades ago. Given the situation, the best approach as already outlined above, is to start at a relatively low adaptation level (e.g. 60%) and gradually increase over time, all the while ensuring that the aids are worn consistently for no less than 10 hours a day (IMO).
I sincerely wish you and your mother all the best
I was just about to write about this—you got ahead of me!
If someone, especially an older person, has gotten used to a quieter world for years, it might be difficult to get used to a more “proper” volume again, particularly all at once. It requires time and some flexibility, which is harder, especially for older people.
Hence, a gradual increase in volume was proposed…
For that flexibility, some mentioned that brain plasticity and a huge amount of motivation are needed.
I am admittedly 35 years old, but I am in a somewhat similar situation. My left ear was completely deaf for a total of 27 years—20 years before cochlear implant (CI) implantation, 3 years of unsuccessful rehabilitation, and subsequently about 7 years of the sound processor being unused. Now I am using it again for 1.5 years, with 80% word recognition score (WRS) in quiet in CI ear only.
With the above experience, I am still getting used to a new loudness in my CI ear. The good news is that it would probably be easier for your mom because she’s not totally deaf.
You are so sweet to write this. My mom’s been wearing hearing aids for about 13 years, since she was first diagnosed with hearing loss at age 87. Those were battery operated hearing aids (Widex Evoke) and were satisfactory, although not fabulous. When she lost one of those 3 years ago, she started looking for the replacement for that, and that’s when this frustration really began. So she hasn’t really lived in a “quiet world,” but more she’s lived in a diminished world, except when she can put the tv on high! I wish you all the best, too.