@DaveL
I actually believe that my move to this area from where we lived was planned for me by my God, while I was happy with the location, and I was getting good service for my hearing it wasn’t optimal. I wasn’t able to hear well enough to serve others by doing volunteer work. When I got here and signed in at the local VA clinic it didn’t have an eye clinic or audiology clinic but I was told it was coming that fall. While my aids weren’t working optimally I was able to wait for the clinic to open. I was the first person that my audiologist saw, we hit it off I got excellent service and I asked to volunteer to do what ever I could to help the clinic. It was like I was intended to be here.
3 Likes
Chuck you contribute so much and have certainly helped me many times.
I see many similarities between sleep apnea treatment and treatment for hearing loss here.
Ontario Canada.
Heck I’ve used rate my doc trying to find a good sleep doc and audiologist. How good is that? It’s not.
DaveL
Chuck, I understand your point and agree that more education is always better, but in my experience there are hearing aid fitters who are truly marvelous - for instance the Costco person I’ve called (on this Forum) ‘the best hearing aid person I’ve ever known’ , who has since moved up the ladder and away - and a PhD Audiologist who fitted me, in 2018, with the most unsatisfactory instrument I’ve ever had (of a well-respected brand/make). No amount of tweaking or return visits helped.
I’m delighted to read of your excellent results!! But I bet that the way you interacted with the VA Audiologist, the way you clearly explained your observations, reasoning, and conclusions; along with the personality of the Audiologist, are more important than simply his education.
Anyway thanks for being a “Voice of Reason” and for encouraging people to keep after their Audiologist or Fitter until the programming is as correct as possible.
Addendum wrt the title of this thread: Hearing aids are better than they ever have been, and I’m grateful! My Grandmother had a body aid in the 1950s… it was a box like a pack of cigarettes with a twisted pair wire ending in a one-size-fits-all earplug. Listening to one’s clothing rustle over the microphone must have been infuriating. My father had all sorts of different hearing aids, none of them worked worth sh*t. I started with an analog Beltone in about 1974 and was ecstatic to be able to hear other people talk, but overwhelmed with background noise… and have had ups and downs since then. So the point Chuck made, above, is quite important - they are aids, not replacements for natural hearing.
And when I start to complain about ‘poor me and my bad ears’ all I have to do is look at the Contacts list in my phone. Half of those people are dead; I have no legitimate complaints.
3 Likes
My audiologist is very informative but I have had many occasions caused him to spend a lot of time on the phone with Oticon, and several times to have an Oticon company audiologist come to the clinic to help with my setup. My hearing loss is a lot more complicated than my audiogram indicates. When I tell people and other audiologist that my aids have 105db receivers they tell me that I only require 85db receivers, will that maybe true for a ‘comfortable’ fitting. But a comfortable fitting doesn’t give me speech understanding, and it doesn’t give me a useable life. It took me and my audiologist with the help of Oticon audiologist 2 years and 15 appointments, 3 different sets of aids, 3 different sets of receivers, and 5 different custom ear molds to give me back my life of being able to hear in meetings, lectures, church and enjoy music. It took dedication from everyone to get it done and it was definitely worth it to me. I seriously doubt that your Costco or many other audiologist would have been willing to put in that much time. And honestly how many people with hearing loss would be willing to dedicate that much effort into it.
4 Likes
Key point there! You didn’t settle for ‘good enough’ (which never really is good enough), you pushed them to get it right.
In my case in 2018 the Audiologist had Phonak on the telephone a number of times, tried all their suggestions, and got nowhere. So it was not really “her fault” and her education was not inadequate, I just got sick of fooling with it and went back to Costco.
I’ll see what happens the next time I go there and have to deal with whoever replaced the person who got promoted up and away. Fingers crossed.
2 Likes
Then maybe Phonak aids weren’t what you needed. Over the years I have tried Phonak, Resound, Semiens, Starkeys, and of course Oticon. Then there was Beltone and Miracle Ear. I never had any luck with anything but the Semiens and Oticon aids. And I never could stand to wear domes, so I wore ITE or Rite aids. And to be honest my first experience with Rite aids was domes and I have my VA audiologist a choice of give me custom ear molds or a set of ITE aids. She chose the custom ear molds which were great.
I think it is the fact that I am a retired IT Professional that was use to push the limits of equipment, vendor and even my customers that gave me the courage to keep pushing my VA audiologist.
And also that my 8 years in the Navy as an electronics technician and later engineer, and part of my Navy career in an agency that had a motto that failure wasn’t unacceptable has been my push for my whole life.
2 Likes
I’d argue that anyone taking 15 appointments per set of aids to get a ‘good’ result is probably not fully comfortable with the software or what the aids are achieving acoustically - hence the calls to Oticon.
I’m assuming that they are running REM with live speech on each adjust to verify the changes made, or at least quantify how you ‘like’ to hear (A:B REM tests on your new/old aids to plot what works better etc.).
Otherwise they’re just using a ‘scatter gun’ approach.
3 Likes
Chuck, there is a saying… that it isn’t the arrow, it is the bowman. Not to say that each manufacturer does not have their own ‘sound’ or idiosyncrasies, but I’ve had a lot of ‘good’ hearing aids (mostly analog) over the years. An analog Starkey wired BICROS ITE set was probably the best ever, overall, but eventually ran out of power as my ear got worse. Before that I had a wired Semiens BICROS that was pretty good, but analog and the off-side BTE just had an ear hook, no earmold/tube, so lying under an automobile made it fall off and drag on the pavement - quit wearing the rig when working on cars.
First digital was a Bernafon from Costco and, although it had too much feedback, it was pretty darned good! I’m told that Bernafon and Oticon are owned by the same big company (that also owns Philips, now) , and that some hearing aid users - once used to their ‘sound’ - hate anything else. I think my current Costco Philips (9030?) is entirely satisfactory; but I also have a ReSound BTE with a plastic tube for backup that sounds pretty good. None of it is good for music or conversation in noise or with masks.
Your background may indeed have prepared you to stick with “getting it Right” - or as right as it can be made - but I’m lazy and “can I live with this?” is probably too lenient.
I never had the pleasure of analog hearing aids, but known what I know do I should have been wearing aids decades before I did.
My dad was Navy during WW2 as a gunnersmate and also underwater demolition. He ran a tight ship as I like to say. He stayed in the reserves and was activated to train the first of the seals. I was raised on a farm and found Navy boot camp to be like a vacation for me.
1 Like
I had a mentor who was a hard hat diver. Canadian
Great man and inspiration.
My Father started as an airman CDN Air Force. Off to university he took Army Officer training. ROTC.
Then became Wavy Navy. Royal Canadian Volunteer Reserve. Off to England as Radar Officer serving on Royal Navy cruisers swinging tothe Pacific at the end of WW2 was career navy. So I was raised as a navy brat.
I think Navy wives deserve medals. Quite the life.
DaveL
3 Likes
I truly believe what you said.
I think that you’re right. Manifestation? People talk about manifestation. There’s much more to it.
Yes any changes of aids, ear molds, receivers, repairs, or even firmware my audiologist has redone the REM checks.
2 Likes
Can you (or anyone else knowledgable) expand a bit on this? I’ve been wondering about what exactly it is about the natural hearing that H/A are not replacing. Assuming they perfectly compensate the frequency dependent hearing loss, what is missing? Why do we have trouble in noisy settings? Why are they not like glasses? What pieces of information are not getting through or imperfectly amplified? What are the physics behind this?
Thanks
1 Like
In a healthy hearing person:
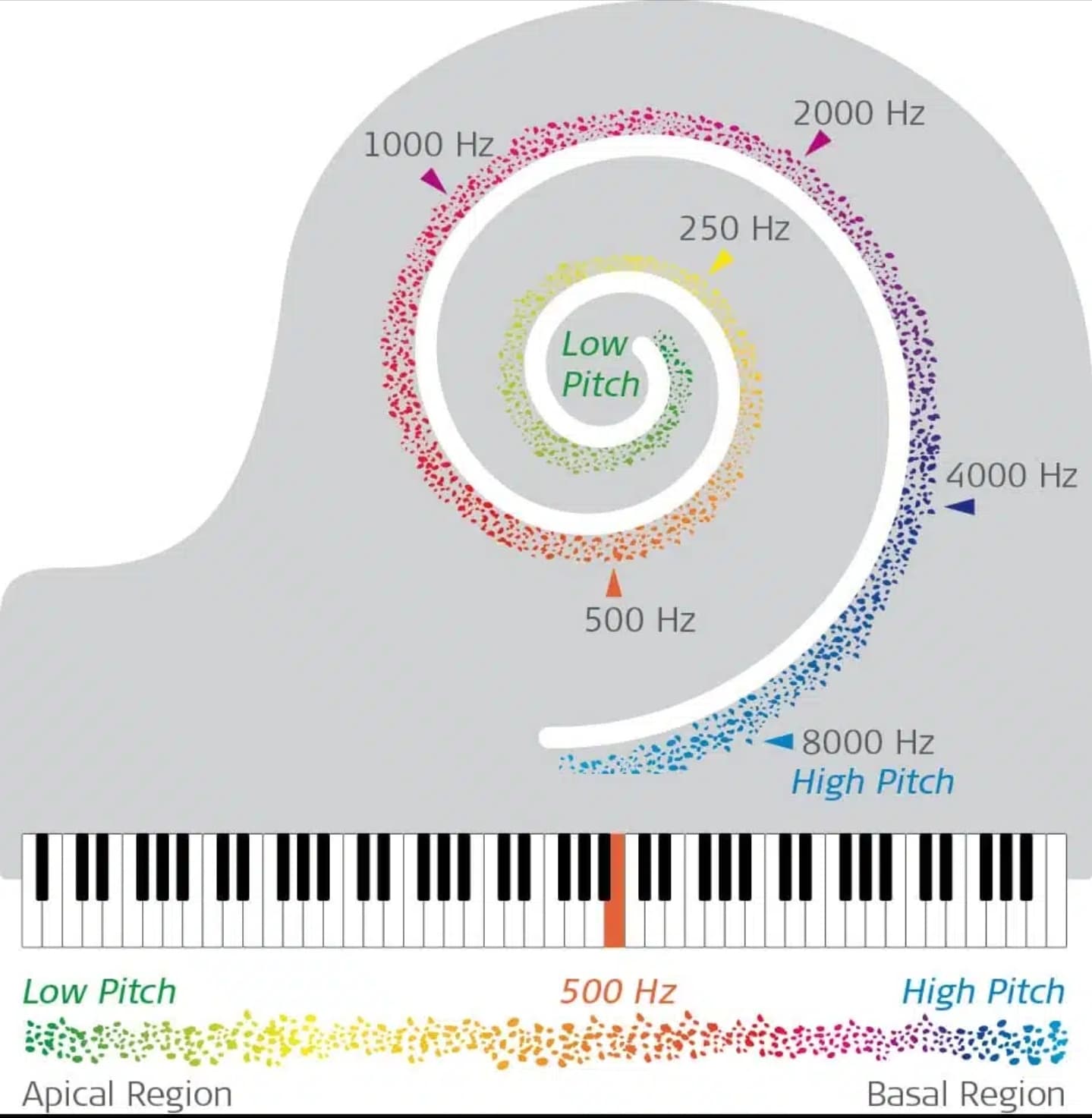
Cochlear anatomy has 3500 inner hair cells and 20,000 outer hair cells. They are arranged tonotopically: in the basal part of the cochlea, they receive high pitches, and near the apex, they receive low pitches.
Outer hair cells act quite as precision denoising devices.
They’re often damaged in hard of hearing person.
That’s because HAs partially replace (imperfectly) function of outer hair cell only not inner hair cell which are final “pitch” receptors and transduces mechanical energy to electrical.
There is currently no possibility with recent technology to precisely replace the function of 20k outer hair cells.
And… There are inner hair cells, which are irreplaceable by HAs. Their death means a “dead spot.” If there is no place in the cochlea to transduce sound mechanical energy to electrical, even the best HA will never provide hearing in those spots due to its mechanism of function.
ABOUT GLASSES:
You’re comparing apples to oranges, because we can compare myopia/hyperopia only to conductive hearing loss than sensorineural.
The glasses simply improve/correct the light pathway to the retina, which transduces light energy into electrical signals. Thus, you can compare that situation to correcting conductive hearing loss.
If you want to compare sensorineural hearing loss to vision loss, you need to do it with retinal diseases, e.g., AMD…
.
- Redundancy of auditory pathway:
- 2 ears
- 2 side of brainstem with neural pathes crossing at multiple levels
- 2 auditory cortex (2 temporal lobes of brain).
EDIT:
I let myself to add the picture from the post below:
END of EDIT.
- Non-anatomical circumstances: auditory training due to continuous processing of many sounds heard.
7 Likes
When we lose our natural hearing and become hard of hearing we loss full range of signal to noise. Meaning we only had a narrow range in which we find it comfortable to hear sounds. We can also completely lose the ability to hear some frequencies and sounds. Hearing aids are just that aids, they can’t replace our natural hearing. But hearing aid technology is improving and with the help of AI hearing aids are improving. I believe the most important part of having different companies developing hearing aids is the different approaches these companies are taking to the same problem. While not all hearing aids will work for everyone with the different approaches hopefully everyone can find an option for their own hearing needs. I know I have found it with Oticon INTENT1 aids. But others will not find the same option and find it with different companies. And sadly way too many just give up or aren’t willing to even try to find what works for them.
3 Likes
The main reason some give up is that you must pay full price to try a HA. That can often be upwards of $5 fo $8 thousand. Granted you can turn them back in within the 30 to 60 day trial but many don’t have that kind of liquidity.
1 Like
Thanks, very interesting, that makes intuitive sense to me. But how does this “denoising device” work? Is there any interaction between the brain and those outer hair cells? How do they know what’s noise and what’s sound we want to hear after all? The points under 2.) (redundancy) seem less intuitively obvious since those facts don’t change with H/A at least not if we still have two years and both are being “aided” by H/As
See wikipedia link in my post. I recommend also second article:
Even though we have two ears, losing some hair cells means losing sensors from which our brain receives signals by neural pathways. Losing sensors means that some neural pathways become less usable, so redundancy decreases.
1 Like
Way back I heard that the brain had to accommodate and learn so that it would accept the hearing aids I wanted to buy. (My response was, yeah sure. I didn’t believe it.)
I waited quite some time to get my first real hearing aids.
Now I have significant hearing loss.I have tinnitus too. My first Phonak hearing aids were magnificent. My second ones were terrible; never set up so I could hear. My third set of Phonaks are finally setup so I can hear. But it’s taken quite a while to get here. I’m very grateful.
Your question is excellent. The responses are too. Ihope my explanation helps. Some day I hope that hearing aids are setup so they work from first fitting.
We all have difficulty understanding speech in noisy environments.
All of us with tinnitus complain.
Musicians complain too.
I thing the minimum standard should be to provide instruments that work in noisy environments, allow us to listen to music. Tinnitus? I just don’t know. If providing noisier sounds, like rain falling or waves on the shore are the solution I think I’ll move to Hawaii to solve my tinnitus problem.
1 Like
My jaw dropped at that question, not because it’s not reasonable but because it’s enormous. I think Bimodal did a nice job responding, and absolutely hearing loss is more like macular degeneration than myopia.
To add to that, for what it’s worth and because ears really are the coolest: The outer hair cells are an active cellular mechanism that ‘sharpen’ the motion of the basilar membrane (the motion of the basilar membrane results in the fluid mechanics that move the inner hair cells that in turn transduce that motion into neural signals) resulting in more sensitive and specific activation of inner hair cells. When your outer hair cells die, not only do you lose access to soft sounds, but instead of a sound activating just a few inner hair cells it activates many (and the effect is worse at higher intensities and with more outer hair cell loss). The analogy I’ve used before is playing the piano with your elbows rather than playing with your fingers. The outer hair cells also receive efferent signals from the brain that adjust their function such that the way your ear works is actually ‘tuned’ by how you are attending to things, and with outer hair cell damage you lose this too. As cells in the ear die, nerve cells connected to them also atrophy and die; the cells in your cochlea are also connected to eachother and send information to eachother to supress or promote signals being sent by their neighbours, and this specific organization is also lost. Cells that make up the auditory nerve are no longer getting all the information that they expect and start to atrophy and die and the signal transmission in the aggregate becomes less consistent with more jitter. All of these changes cascade up into the auditory system, and additionally if someone goes without amplification for a significant amount of time (as most people do before getting hearing aids) the auditory cortext starts to lose some of its frequency-specific organization. At the end of the day, as hearing loss progresses you don’t just lose the ability to hear certain soft sounds, but you also have reduced frequency acuity and so more smearing, you lose the ability to engage in auditory scene analysis and pick sound out of noise, you lose sound localization. There are a ton of supporting cells in the cochlea as well that do different things, and so individuals can have similar thresholds that actually reflect completely different disease processes in the ear which impact all of these auditory skills differently. It’s not a basic physics problem, it’s a biology problem.
I shouldn’t say “all hearing aids can do is turn up the volume” because modern hearing aids are doing all sorts of things to try to support the damaged system. But it’s a damaged system, and as of yet we have no way to repair it. The other way I some times think of hearing aids is. . . imagine you have a broken speaker and you can manipulate the audio that you are sending to the speaker to try to make the output better, but you aren’t allowed to actually fix the speaker.
7 Likes