High-level otologists keep telling me that my right middle ear being chronically filled with fluid has no impact on hearing clarity in someone with my profound sloping SNHL as long as I have proper amplification. They use this to avoid having to consider other possible treatments to actually reduce fluid, in addition to hearing aids. I get their concept, but I believe it neglects some important factors. I imagine that the increased (by 35db) amplification across frequencies would in and of itself decrease clarity and cause other issues like feedback and more difficult fitting constraints? There is also the occlusion effect (own voice difficulties), feeling of fullness and who knows what else. All my problems were caused by radiation and cisplatin for head and neck cancer at age 27. @Neville @Um_bongo @Louie
I’m certainly no medical expert and hopefully those users you tagged will chime in eventually.
- Have you tried (or are you using) hearing aids yet? No you would get increased clarity with hearing aids. How could you not?
- You’re making several assumptions with the feedback, more difficult fitting constraints comment. That’s why I asked if you’re currently using hearing aids.
- Occlusion is experienced differently by people. The feeling of fullness is also subjective. The own voice “problem” I think is all about oh…my voice is out there in the soundscape and the aids are hearing me speak and amplifying it. Rather than the internal vibrations of you speaking, the aids are hearing you. You get used to it.
For my experience, I also always seem to have fluid. I somewhat frequently blow out my ears (valsalva) and often get internal bubbling sounds. But I do eventually blow through and suddenly I can hear much more. Always be careful with valsalva. Only push as hard as you’re comfortable…or stop when you faint  and stop immediately when through.
and stop immediately when through.
I use vented domes to counter what I think is meant by feeling of fullness. I call it built-up pressure in front of the ear drums/behind the aids which I find uncomfortable. I was first fitted with closed power domes. Never again. I ripped those right out immediately.
This is THEORETICALLY true, but they are missing an understanding of the limits of amplification. Tube placement is a very minor surgery–is there a reason they are trying to avoid it?
I’ve been untreated (no HAs) for 2 years due to the insane incompetence and negligence of my local VR office. Before that I had opn1 that were never properly fit. Lumity L90s have been ordered, but now the audiologist is screwing up the earmold order and being extremely difficult. I’m thinking that titanium C-Shells would be the best bet.
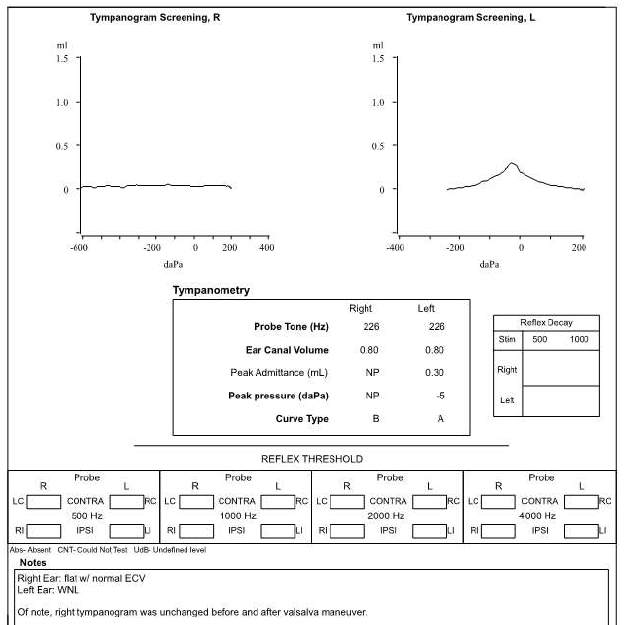
I’ve had a pretty severe own voice occlusion effect, fullness in right ear and type B (flat) tympanogram for a year that has nothing to do with hearing aids and everything to do with fluid.
What are the risks of Valsalva? A couple treatments that seem to really be helping with the fluid are Johnson baby shampoo sinus irrigation, and Atrovent nasal spray. Others that are promising: N acetyl cysteine nasal spray, mometasone irrigation, guaifenesin, and balloon dilation.
I believe my chronic eustachian tube dysfunction means that PE tube placement would only help until healed. I’d be very interested to hear more about what you mean by the limits of amplification (in regards to fluid)?
I have a similar middle ear fluid issue that can sometimes cause my right ear hearing to go from decent hearing to quickly shutting down to about half. What I have learned to do is remove my right hearing aid and gently push the outer ear several times so that I can actually feel fluid swishing from my middle ear out through my Eustachian tube .
This temporarily clears up my blockage. My ENT has told me I am doing no damage, but usually provides ear drops to help clear up this issue.
When I get head colds it’s even worst, and end up pushing my outer ear several times a day.
That’s interesting, thanks for sharing that idea. My otologist has said that the eustachian tube doesn’t typically drain. The middle ear tissue releases and absorbs fluid based on the pressure within it. Based on that, it sounds like your technique could worsen that problem.
So. . . permanent tube? ET balloon dilation?
There’s an upper limit to the gain that a hearing aid can provide which is a combination of the most powerful devices on the market and the physical fit of the earmold in your ear to manage feedback. I don’t know how your hearing aids are fitting, but I would guess that there is some critical information available to the left ear between 1-2 kHz that the right may not be providing. But how do you feel? Do you find that, when aided, you’re getting just as much out of the right ear as the left?
Balloon dilation would not be worthwhile if ET is too scarred by radiation (most otologists have insistently assumed it is). I have two concerns about permanent tube: I’m an avid underwater swimmer in rivers and oceans and wouldn’t tube/perforation compromise TM function to some degree?
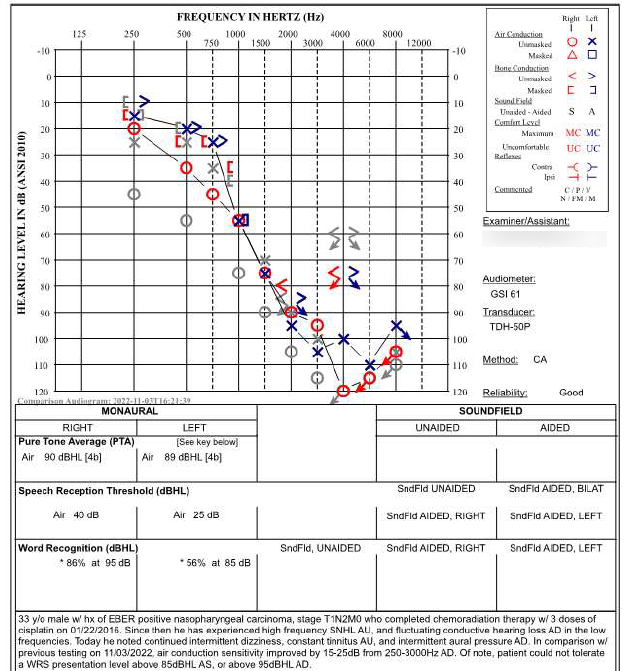
My worst threshold 1-2khz is 105db. Is that too close to upper limits of amplification or is there some other issue with fluid causing a loss of information?
The following testing was done on an unusual day (1/5) where I went out of my way to introduce max amounts of air to middle ear and consequently noticed very significant (yet very temporary) improvement that is reflected on audiogram. Improvement was despite persistent type B tympanogram. Any other plausible explanations for my type B tympanogram other than fluid?
So, if both treatments are out for you, then you are just left with hearing aids. However, I would expect the right ear clarity will not match the left.
However, if you were able to get that fluid out. . . You could try something like the Otovent and just use it regularly to try to get ahead of the fluid issues.
I’m not saying that either treatment is out. I just don’t know anything about how effective or necessary swim ear plugs are for jumping into rivers if you have a perforation, and I don’t know whether tube/perforation would compromise TM function to some degree?
Is there any benefit to Otovent if you are an adult that feels very comfortable with Valsalva?
“I would expect the right ear clarity will not match the left.” The reason I created this thread is to answer why you would expect that
“This is basically the same question: My worst threshold 1-2khz is 105db. Is that too close to upper limits of amplification or is there some other issue with fluid causing a loss of information?”
Yes, there is truth to what you’vebeen told. Unlike a sensorineural loss (inner ear/nerve damage), middle ear dysfunction doesn’t compromise the quality/integrity of the signal as it travels to the brain. The inner ear is what converts the signal into electrical impulses to be sent to the brain, so damage in this area inherently compromises the signal. The main function of the middle ear, however, is to amplify the signal via mechanical processes. In the presence of middle ear dysfunction, the role of a hearing aid is to provide enough amplification to overcome the dysfunction and ensure the signal arrives at inner ear with sufficient volume. So, for example, if someone has a moderate loss that is entirely caused by middle ear dysfunction, we often see that they do very well with even the most basic hearing aids.
With that being said, everything @Neville said is also true. If the total sum of amplification required is such that you are likely to run into feedback issues/restrictiond, or near the maximum output provided by your hearing aid, these factors can limit the benefit obtained by hearing aids. I hope that makes sense. Sorry for the late reply
Could you speak to this in my particular case? I am ordering Lumity Life 90 and will ensure that I get well fit earmolds. I’m thinking titanium C-Shells.
One thing that has never made sense to me about what you’re saying is that it seems like when you have fluid in middle ear or ear canal or are underwater that you lose a lot of clarity in addition to volume. It changes the subjective quality of sound drastically, not just the volume. This seems to be roughly equivalent to the theory behind hearing aids and fluid (correct me if I’m wrong): If you were underwater in a pool and someone played audio with sufficient volume and equipment and also equalized it to make up for the specific frequencies attenuated by water, then it would sound normal to you? Thanks!
Well reduction of volume in the high frequencies is often what results in a perceived lack of clarity, and being under water will naturally result in an overall reduction of volume across all frequencies. Yes, if you somehow overcame the impedance of the water so that the sound arriving at the inner ear was normal, you would hear it no differently to if you were above water… as absurd as that seems
The middle ear transmits sound through direct contact from the eardrum to the ossicles to the cochlea. If it’s filled with fluid then transmission will be damped by the fluid. But transmission is still via direct contact, not via the fluid like when you’re underwater.
The middle ear issue seems to be pretty marginal in terms of the overall loss. There’s a bit of variability caused by the conductive element, which is probably making the fitting more difficult.
It’s a bit of a pig of loss in any case, especially if there’s a problem with louder speech.
Even with maximum frequency shifting/compression the effect of the downward spread of masking is going to be huge, so you either accept that and shut down the upper frequencies to an extent or you have to live with distortion and Feedback across all sounds.
Could you give more details about what you mean by this?
Would you recommend max frequency shifting and compression? Would those be 2 different types of settings with Phonak Lumity? What frequencies would you consider shutting down?
Do you tend to recommend/prefer titanium C-shells? I know the downside is no modification, but given past experiences, I want to avoid modifications anyways.
Thanks!
The point about louder speech is that you might run into distortion/feedback even under normal amplification conditions.
As to the optimum set-up, I don’t do Phonak. The titanium shells don’t have a very good reputation, but as long as they stay together and they fit, then they’re not a bad option.
Your 4-6KHz is pretty much shot though. I wouldn’t be surprised if there’s a deadspot there.
Any particular reason you don’t do Phonak? Why does titanium have bad rep?
So I gather that 3.5-4khz would be the range that would be difficult to decide whether to shut down or not? Anything I should do to diagnose/treat a deadspot? Thanks!