In December, an audiologist still said 1/3 gain for SN loss and 1/2 gain for Conductive.
Over a certain volume more hearing damage occurs, therefore gain must be limited to prevent that from happening.
I’ve never know a digital hearing aid to put out 50 dB of gain for a 50 dB loss.
Hearing aids, aid, they don’t give us normal hearing.
This is mine. Not sure what I think.
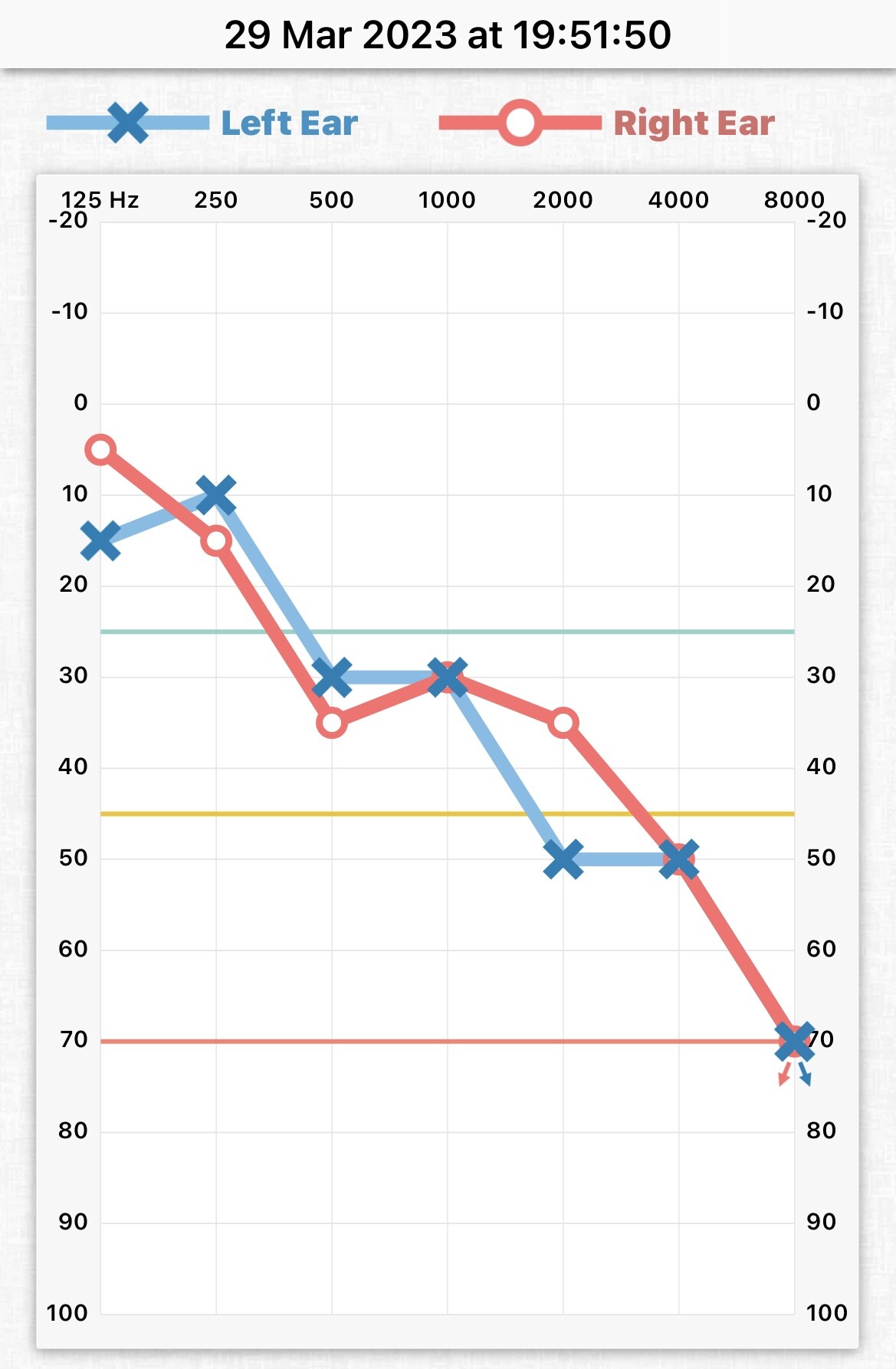
You’ve got better high frequency hearing with the hearing aids. Wonder why I haven’t?
@tenkan I realise this isn’t accurate but could I potentially get more benefit from my hearing aids? Would you know?
Oticon Xceed 1 UP.
People with sensory-neural hearing loss have a reduced dynamic range. The objective of the hearing aid is to make maximum use of the available dynamic range (in each frequency band) to try to restore hearing (usually with the target of maximizing speech comprehension) as much as possible. The hearing aid output for medium sounds falls a somewhat below the middle of the available dynamic range, with variations depending on the fitting method used. For very soft sounds, usually you are not interested in the humming of your refrigerator and other machines so usually a higher floor than 0 dBHL is used (with techniques such as expansion), that can be adjusted to the preferences of the user. For high volume souds, as I’ve already said, you won’t add any gain once the hearing damage threshold is crossed.
For loud sounds on my hearing aids, it’s in the 40+ range. None of my frequencies say 0 on them.
I’m really confused as @Um_bongo a qualified person, says 1/3 gain still.
1 Like
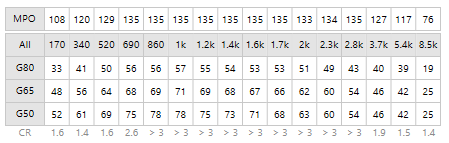
This is my friends settings in Target as it is easier to see then Oticon.
None of her numbers say 0 either.
Have I completely misunderstood?

To better understand all of this I recommend you this reading:
https://www.amazon.com/Compression-Clinicians-Compass-Hearing-Fittings-dp-1597569879/dp/1597569879/ref=dp_ob_title_bk
1 Like
Oh wow. Yeah I see what you mean… I wonder if maybe because your audiogram is worse than mine so perhaps not pushing it up as much? I am not 100% educated I know but is severe high frequency loss harder to fit? Have they ever said about cochlear implant?
What app did you use? I will be interested to try it as well and compare with the one I used before (Audiologica), an app on Google Play.
Lovely, my ears are 75 years old!

My hearing has been made worse by Chemo. I’m not getting a cochlear implant due to being told I’m living a max of 9 years more. I’m in my 30s.
I am using Android and cannot see it on there, maybe they do not do it on there?
You cannot hear high frequency sounds with your hearing aids in? So what you are hearing now with your hearing aids is similar to what I hear without cos it looks similar to my audiogram.
I have been learning about inner and outer cochlear hair cells. You need to have good inner hair cells for hearing aids to do their job. If they are damaged as well, cochlear implant is the best option.
I just do not understand why in the UK they do not do Word Recognition Scores like they do in US!
Is that what they said? Your quality of life is STILL important and hearing is a big part of it… so sorry to read what you are going through. Similar age to me as well.
Any output (output = input + gain) over the MPO has 0 gain.
I’m barely into this thread but I have to disagree with the others: your questions are entirely reasonable. And, frankly, the answers so far are less than satisfactory. Maybe the thread gets better!
Depending on whether you have sensorineural loss OR conductive loss, and what type of this last, HAs can help to a greater or lesser degree. It’s somewhat complicated, but the important thing is to find out what sort of loss you have, and what are the best options for ‘restoring’ that loss, or working around it in order to help you hear speech and music as well as you can.
My hearing loss is entirely conductive. My auditory nerve is perfectly fine. I may have some loss in the hairs for hearing in my semicircular canal. HAs can amplify the heck out of sound of high frequencies, where my worst loss occurs. But it’s my ear drum and middle ear that are all messed up–I have conductive loss. All of that amplified sound can’t move much beyond that blockage. Although some can…it’s tricky and very individual.
I have a bone assisted hearing aid–BAHA–for this ear. Since my auditory nerve is fine, that circumvents the middle ear and sends sound directly to the nerve via the mastoid bone. This was a simple surgery to implant the device on the outside of my skull, just under the ear. Nothing very invasive! For some folks, this is a good option. Lucky me, traditional aids work pretty well too.
It’s not just about the HA devices. they can only do so much. All of the major brands will pretty much perform the basics equally well. There isn’t a magic brand that can restore hearing loss that’s the others can’t. (wait, with this caveat: if you have extreme conductive loss and a functioning auditory nerve, a BAHA device CAN restore an astonishing amount of hearing. Check out some of the videos of young deaf children having their BAHA devices activated. It truly moves the heart.)
It’s important to understand the causes of your loss, in order to find the best option for addressing that.
![]()
She/He is asking about how the gain works within hearing aids, not what hearing aids are best!
Be note, we are not professionals.
The professional in this thread has answered very clearly!
2 Likes
Honestly? ……behave.
It’s answered above.
We get a thread like this every couple of years, someone thinks they’re the first person to encounter gain modelling wrt their loss. As Zebras said, it’s roughly 1/3 gain for sensorineural and roughly 1/2 gain for conductive losses.
I appreciate you’re the first person in your immediate experience to encounter this, but (sorry to say this) you’re not the first person your audiologist has fitted this week with the same underlying loss. Now, hearing loss is massively personal and subjective, but the person who is testing you is doing it from an objective basis: that might de-personalise it for you, but thems the breaks.
Please, embrace the science, engage with a fitting professional that you respect and develop an understanding of how the fitting algorithms didn’t just land yesterday; even though it might not quite fit with your expectations of how Hearing aids should sound.
4 Likes
wow. where did all of that come from?
Behave?
Maybe you’ve accidentally responded to another poster?
wasn’t there a rocket sent to Mars some years ago that missed its target–or maybe the whole planet–because some scientist forgot to convert American measurements to metric? I can imagine an audiologist lecturing his patient about how he must behave and accept the metrics he’s being shown that prove his hearing aids are working fine, even though the patient ‘thinks’ otherwise. (“thinks, schminks”, thinks the scientific audi. “what a rube”…). I can also easily imagine that a year later, another audiologist determines the first had made a gross mistake in their measurement and adjusts the HAs to great benefit of the “rube”.
Them’s the breaks? Your subjective experience has to shut up and behave? which audi has the definitive proof? Hmmmmm…
More proof then you!
More training then you!
More honesty than you!
You attitude on this thread is rather shocking!
2 Likes
He is a successful, respected audiologist who runs his own hearing practice for years. What are YOUR qualifications for making such statements and demands??
I think @moderators need to review your posts in this thread and handle accordingly.
1 Like
Oh come on guys! I’m the one under attack here. quite shocking? I merely requoted what Um Bongo said to ME. How is that “shocking”? Zebras, my example was imaginary. You’re telling me that one of my imagined audis was far more experienced than the other imagined audi, who correctly read an imagined chart. and then you attacked me by saying the first imaginary audi was “far more experinced…had more training…etc.” than me.
Again: both audis are imaginary. So is the patient, in my “for example”.
Puhlease.
Oh, and nowhere do I make any demands.
What in the world has got into y’all?
I said that I found the OP’s initial questions to be reasonable. Somehow you find this shocking. Again, Puhlease.