Because you have to say yes to a tone? Just like you already did during the audiogram? This is the weirdest logic for arguing that in situ is better.
2 Likes
AFAIK all those are forms of REMs. There’s not just one REM but if I remember correctly like 8 of them, no?
Check here what I think should be covered, under tests:
I also always try to emphasise that I think about REM based fittings using speech.
Which are the only ones that seem relevant for actual fitting and getting WRS out of HAs as per expectations.
When my fitter starts, he does several things before we get to speech part. From what I’ve gathered, all those are various REMs.
Is it possible that @Um_bongo and @TrueBrit you’re screaming against REM with noise, while I’m screaming for REM with speech all this time?
Eg that we’re basically screaming for the same thing but terminology got lost in the translation?
From here:
https://affordableaudiology.com/real-ear-verification
So what is it at the end, live speech mapping is using REM or not?
This tells me that yes, or?
@Neville which one you think when you say REM fitting?
https://blog.valuehearing.com.au/news/dont-1-3-ends-not-using-hearing-aid
They say that 1 in 3 people don’t use their aids (based on some study).
For me that’s a proof that all those fitters don’t deliver useable results.
I knew only one other person in real life who got HAs, and after several fittings, she just put them in the drawer, she was too tired of guesswork and they didn’t helped her.
But let’s first sort out terminology ![]()
The two situations are totally different.
OK, let’s stand back a bit and review the situation from afar,
-
The first in situ system I know of is the Widex Sensogram from 1996.
-
In-situ systems are still being used today, by almost every manufacturer.
-
As far as I know, nobody has ever suggested replacing the standard hearing test with in-situ tests.
Taking all this together, one can only assume that:
-
in-situ tests perform a useful purpose
-
in-situ tests are not equivalent to standard hearing tests.
I’m not sure what your point is with that. I am not saying that an audiogram and in situ measurements are the same, what I’m objecting to is this idea that in situ somehow “involves you” in a special way that makes it better than REM. In situ provides a measurement of how the fit of a particular hearing aid in the ear impacts detection of a sound relative to the standard audiogram. REM does the same thing with a more direct measure–“involving” the patient a second time doesn’t make any difference. And then beyond that, REM allows you to confirm that the hearing aids are actually doing what they claim they are doing, which in situ does not (which also, on a group level, allows for the development and refinement of prescriptions and the advancement of our field). As far as I can tell, this “in situ involves your brain and processing” is a nonsense feature that was probably developed for marketting. But maybe we’re just not communicating clearly and I actually have misunderstood your original point.
To me REM is anything that involves putting microphone next to the eardrum and taking measurements using an independant, calibrated instrument. There are various measures that can be taken for various purposes, some more or less useful depending on the context.
2 Likes
wow, thanks for the discussion.
I think the majority see REM as a starting point. It also makes perfect sense for me to choose a starting point that is objectively ok.
I had to replace the cables for the rics, because these were too short. With this short cables and in-situ @home revealed that all the tones were too quiet. A fitter should see that i think.
At the same time, I once again started the discussion whether REM would bring something or not. His arguments were that the manufacturers’ formulas were secret and that he could not verify the result. I said okey, but he doesn’t have to verify it. Oticon’s Genie software provides an interface for the Aurical System and processes the feedback automatically.
After a while we made the test and he compared the result from the HA with NAL-NL1. He wanted to prove me that the manufacturer’s formula is okay. Clearly there were deviations, which according to him, are of no consequence. braindead
And why should even Oticon advocates REM adjustment and add extra functions into the software when it is pointless?
A question that my fitter cant answer ^^
I will discuss it again with my ordinary contact on Friday. I’m curiouse how it work out. I always try it with step-by-step arguments, but REM seems always senseless in this company and program the HA as it is convenient for the customer.
The best thing is always ‘how do you hear me now’ what Blacky mentioned.
Last time I didn’t hear a difference if I wasn’t focused on it. Which was also called “great” because then the sound is not intrusive. A mindset that I don’t understand.
What do you think about an open supply? I think closed is simply better, because the entire filtering of the hearing aids works better.
Really not sure what you mean by “open supply?” Are you talking an open fit vs a more occlusive fit? If so, advantages of open fit are a more “natural sound.” Disadvantages are that not as much gain can be applied, especially at lower frequencies, more issues with feedback, noise reduction systems are less effective. More occlusive allows for more gain with less feedback and more effective noise reduction at the expense of possible “occlusion.” More occlusive has many advantages but depends on how well the individual tolerates the occlusion.
That’s true.
Verification is available only for those formulas, NAL, DSL and such.
What is weird is that he thinks that he should fit by manufacturer formula and not NAL-NL2.
However, one think what I’ve found for phonak marvel/paradise is that if you pick non manufacturer formula in HA (and then you can do REMs) you won’t get one thing - different attack and release times. They’re available only on their proprietary formula.
I forgot which setup they’ve chosen to implement, fitter doesn’t have the ability to influence that. And I don’t know what is the default for other formulas, I just remember reading their article about attack and release time and realising that they intentionally didn’t implement that on other formulas, only their own. Bastards ![]()
Goggle ‘attack release times phonak’ and you’ll find it fast.
But also, finding is that those other attack release settings aren’t for everyone. So, I’d say manufacturer formula (for phonak) might maybe have sense to use on group of customers for which that was shown to make a difference, while on everyone else should regular formulas be used, since they can be verified.
Edit
NAL-NL2 has more bass
NL1 has less, and is more focused on speech, but was changed for NL2 because people weren’t happy with it
In my case where I want to completely remove bass to remove distortion it brings, NL1 did better.
Here is the dilemma I have with REM vs. Manufacturer first fit vs. Insitu. from a clinician point of view
prior to my current role I worked for years with Widex, who strongly promote the sensogram (in-situ measurement). When completed correctly this measurement typically provides a much larger low/mid-frequency response compared to what Nal-NL2 recommends. Furthermore, unless a fairly closed fitting is completed Widex, with its traditionally poor feedback management (cant comment on latest chip as havent fitted) could certainly be adjusted to ‘match’ target however this requires deviating heavily from the Widex recommended sensogram settings and matching the high frequencies meant that the aids became very unstable (imagine two chirping canaries sitting on top of the ears)
Moving forward I now work with Signia, Resound and Phonak/Unitron. Phonak prescription tends to be fairly close to NL2 targets, Resound isnt too far off either. Signia however is way off, in particular when open-fitting.From what I can see their proprietary prescription tends to provide a lot less gain, particularly for an open fitting first time user. Once again I can easily match target, however when I do the patient complains that the aids are way too sharp and loud. In fact, the proprietary Signia formula tends to get the most consistent positive responses from the patient.
I always run REM / Live Speech Mapping for every fitting, but the dilemma I face as a clinician is what do I choose? Do I fit to what the manufacturer has researched themselves (and likely set up all parameters of their aids to work based upon that research) or do I push the hearing aids to match target, but then have to potentially compromise on patient comfort and their own preferences for sound quality. I cant help but worry that when I am making significant adjustments to how the manufacturer software sets the aids then those aids are really just moving further away from what is going to work best for the user based upon manufacturer design.
Anyhow, I suppose there’s no real answers to any off my questions because user perception of amplification is very subjective. Personally I end up fitting hearing aids based on a bit of all of the above - but always trying to provide the user with what I think will suit their preferences in the best possible way.
12 Likes
My fitter said that widex can’t be fitted with rem 
My conclusion is that they heavily process the sound or something.
I’d say best approach is to measure WRS without aid (on headphones and whichever db are needed) and then use whatever formula is needed to achieve at least such WRS with aids and sound at, what, 65 dB. In quiet, through the speakers.
Also ask client if they want comprehension or comfort.
In case they don’t care about comprehension, then not chasing WRS is fine.
But if they want comprehension then hitting WRS is a must, but doesn’t need to be done at first time, so adaptation and slowly pushing someone into their targets.
Also, for flat loss or high frequency sloping loss but not too steep ones, it is probably equal whatever you choose as starting point.
But for anything complicated, I’d definitely start with non manufacturer formulas first.
Neither widex nor phonak manufacturer formula worked on me, even after some tweaking. Widex worked but tweaking was insane and long, so end result didn’t have any resemblance with the original curve and I wore tulip dome.
When other person tried, again starting from manufacturer formula and vented mold, and a bit tweaking - results after 2 months was that I hear better without that aid than with it.
Whilst phonak rem fitted (speech mapping) on NAL NL2 and vented mold was miles better than anything from manufacturer (both phonak and widex), but still, worse than my target WRS. What hit WRS was NL1 and open dome, believe it or not.
Maybe he doesn’t know where you can change the formula in the genie software used by oticon.
Stil, I can’t understand the argumentation.
Even with the oticon formula there should be a visible change in the
target view. And that should prove him wrong?
Maybe i should leave and try it somewhere else.
I don’t know if Genie supports REM measuring for speech mapping, for that it’s usually used the SW from the measuring device.
But yes, geanie should support choice of formulas and then you pick one on aids, pick the same on the verification sw and run it.
Phonak adapts targets also directly in target sw when you switch between formulas, eg gives you gains as they calculated.
But, it is definitely worth investing time into finding fitter who follows best practices summarised by dr cliff.
Maybe it’s cumbersome at first to filter them out, but will save time, nerves, energy and money.
I’d call, send email, go there, whichever is easier for you and ask what beside audiogram they do to ensure that they’ve fitted aids to the best of their ability for your hearing loss. And then listen. If they don’t mention stuff, you ask. If they try to say how it’s not needed, or obsolete, say aha and end the call, not worth the time.
My last fitter did REM on my Phonak Naida B using NAL-NL2. With this approach the highs (>2kHz) were much too loud. And even loud noise at around 1kHz was still too loud. After I bought those aids I did insitu with NAL-NL2 for myself. It was better but still bad for loud input (G80). With DSLv5a and especially APD/C (manufacturer’s formula) it was ok as a starting point. For me.
In short: REM is not a holy grail. It can be a starting point. But the more important thing is that a fitter has to carfully listen to his patient and know what the hell is going wrong.
2 Likes
Part of the issue is doing the REM to a target rather than a weighted Speech level.
The other problem is that within NAL/DSL etc, there’s competing ideologies in place in respect of whether all parts of speech deserve equal prevalence and amplification.
Another problem is that the stimulus tones used are often identified by your HA as gibberish, so they don’t turn the sound up as they do for speech.
Anyone who is adamant that this prescriptive system is the only way to go either hasn’t fitted that many hearing aids in the real world or is just a fanboy of a particular REM system. Used judiciously REM is very helpful, but just like driving a Tesla and not looking at the road, if you blindly rely on what the machine says, you’ll come unstuck at some point.
5 Likes
I don’t think anyone is saying REM is the best way to go, but I think it’s way better than using the Quickfit approach as a starting point.
I’m really new to the hearing aid business and I’m trying to find some good aids. But 2 out of 3 “fitting experts” have never checked how much of the sound is reaching my eardrum. In addition, one was surprised that I have problems when the ric cable was too short/long and the open mold does not radiate well into the ear canal.
For these cases and for control, I see it as a good way. Above all, an inexperienced person does not know which frequency range is important if he has not heard it for a long time.
A problem with this “how can you hear me” approach.
My Costco fitter set up my KS9’s with REM. I didn’t like the result. I went back for what I thought would be a simple change but was still unhappy with the result. So I bought a Noahlink Wireless, made some DIY silicone earmolds, reprogrammed my aids with Audiogram Direct and am very happy with my current fitting. The KS9’s are the third set of aids I’ve programmed with AD and all have worked well.
It may be that my lack of technical knowledge means that I’m missing some potential benefits of my aids, but my main goals are to understand my wife and understand dialogue on the TV. I’m happy with the results from my reprogrammed aids. (age 80)
7 Likes
The VA uses REM. They seem to have complete faith in it. I was told by an Audiologist there that they only use NAL/NL2. When I asked about DSL5, they said it was pediatric only, which isn’t true. But, if they only use NAL/NL2, they might not know about the adult version of DSL5, which I prefer to NAL/NL2. REM doesn’t work for me. My recruitment makes a REM fitting unbearable. I have seen mention of doing REM fitting while using SR2. That might work, but I doubt it, because of the recruitment. I agree that REM is a good starting point, and works well for a lot of people. Phonak says that Audiogram Direct has been tested and proven to be an accurate method. I have reservations about it, but used it for my own fittings.
Curious if you know what differences between the fittings or audiogram were? Was there a bone/air gap on your Costco audiogram?
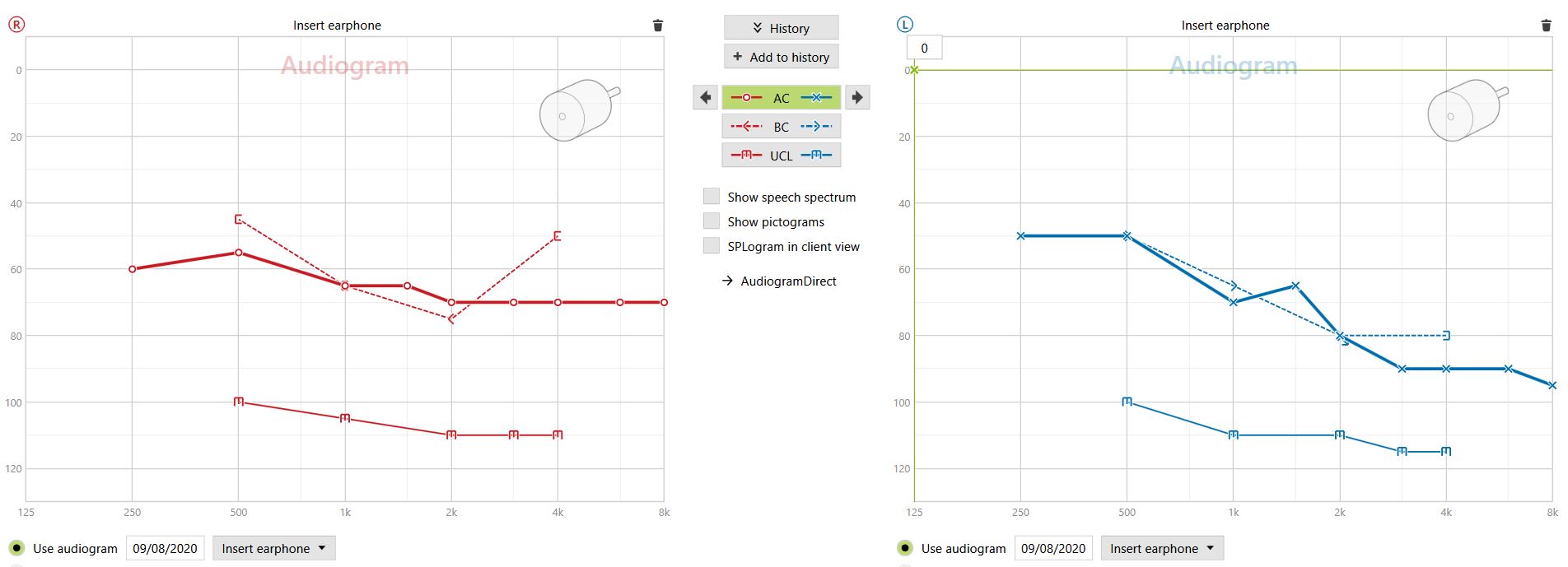
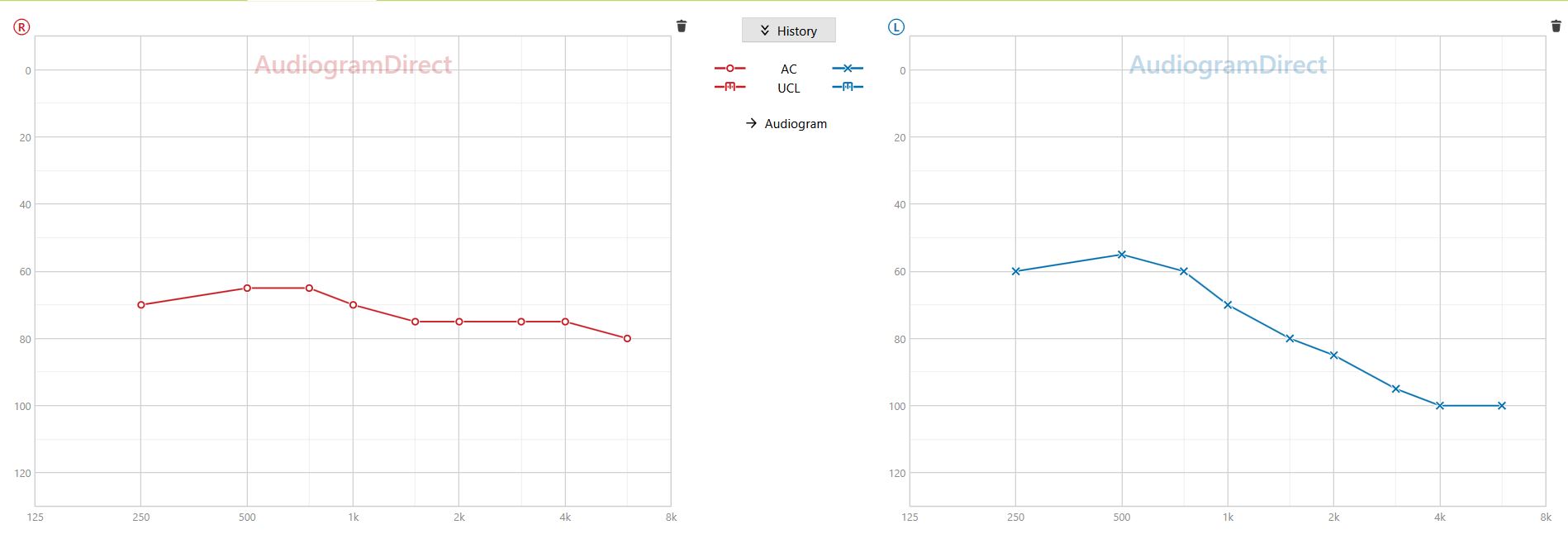
You don’t have a bone/air gap. (It refers to a significant difference between the two different types of tests they do) Really don’t know why you’re so much happier with your fitting with Audiogram Direct. The audiograms are very similar.
There is a good 10 dB difference across the board that I can see. The Audiogram Direct has a little more detail.
I would suspect the original fitting was very loud to the OP. The details in especially the left Audiogram Direct fitting could really help speech IMO. Better details in the right too.
Glad the OP is happy.