Hoping I’ll qualify for a discreet one.
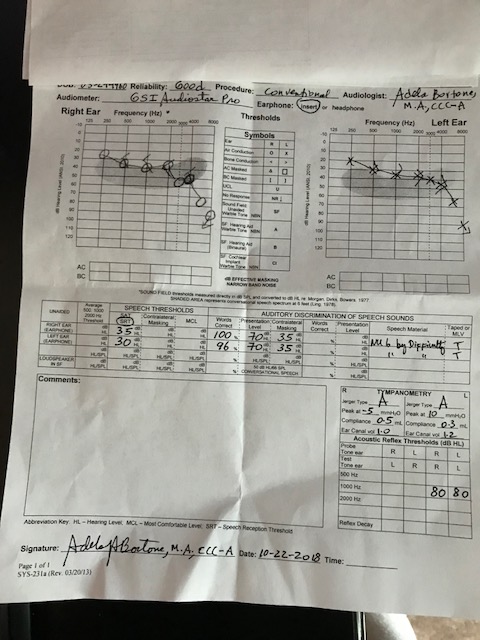
I can’t read that. Looks like it might be mild to moderate hearing loss? Probably any brand will work. It is important to find a pro you like and trust and work with them on the style and your preferences. Also, it takes some time for the brain to get used to the new sounds. It is not like getting new glasses and seeing perfectly well. With hearing aids it takes some time to get the full benefit. There is usually a return period where, if the hearing aids are just not working correctly, and the pro cannot seem to get the problems worked out, you can take them back and try another brand or pro.
1 Like
Hi pati,
This video is a good one at explaining the differences between the different hearing aid styles. If you look for other videos by Doctor Cliff, you’ll get a lot of good information.

1 Like
I wouldn’t consider fitting any sort of ‘canal’ aid to that loss so it all depends what you mean by discreet. Small RIC would be great for it.
FWIW why are these audiograms handwritten? Computerised audiology has been around for nearly two decades? Surely people aren’t still using kit from the last millennium?
1 Like
My audiologist office trains doctoral students from the nearby schools, and uses handwritten audiogram forms.
Oh yeah. NHS England still do handwritten audiograms! Had one done recently by the NHS in London ![]()
Agree re RIC.
It’s just backward, the kit has been around for ages - part of modernising NHS audiology in the early 2000s was based around the introduction of computerised systems - the GN/Madsen Aurical was available at the time.
The reason why it’s so exasperating to see the regression to paper is that if the test audiogram is done by this method, there’s fair indication that the values are manually entered into NOAH, and likely that there’s no REM system in place to verify the fitting.
Using handwritten systems within a teaching environment is bordering poor practice - unless there’s an underlying justification to let the students see how to build an audiogram and implement the rules of masking etc.
2 Likes
Yeah. It’s still manually inputted for tuning and fitting purposes in most places within the NHS. I’m going private now and getting OPNs in November. I have already had a hearing assessment and this was done on a computer so all good! ![]()
Also, I think it’s to save time. The audiologist that did my last hearing test was clearly stretched for time with very few resources. The cuts that have occurred over the last few years are very clear to see, especially in adult audiology.
I disagree with the former comment about not fitting a canal type aid. Your hearing loss is an easy one to fit and the type of style is pretty much open. The critical factor will be the size and shape of your ear canal if you want a CIC or Canal style aid. The venting and occlusion control available today have opened up the small hearing aid styles to many more people. The biggest problem going small in the canal is the lack of room for directional microphones, and directional microphones do help in background noise. If you go for a CIC fitting, I would not get the premium level instrument since without directional microphones some of the advanced features are not as effective. You should do very well with amplification. Good luck!
Fair enough if you want to disagree with it, but the size of the vent hole needed to accommodate a 20dB LF loss (without occlusion) is likely going to be bigger than the possible venting down the side of a CIC/IIC even with a notch/Iros.
Why create an acoustic problem when there doesn’t need to be one?
Some people are just happier with the small instruments. Patient satisfaction is the main concern. I have seen people who will not wear anything behind the ear, IIC, CIC. or mini canal instruments are all they will accept. Something post-auricular may be technically better acoustically, but if it is not worn it will be of no benefit. I know of some practitioners who are still fitting 80% CICs and have happy patients. The main reason for disagreeing is that I would not patently rule out the small style without know more about the patient. In reality I am in your camp and if I was fitting this patient, the small custom products would not be the first thing I recommended but it also would not be ruled out.
I’ve had two audiograms. First one was performed by a doctor of audiology and was handwritten. Second one was done by an HIS and was digital.
I’m with you, I am surprised when I see handwritten ones.
All four that I’ve had done were hand written. From 2016-2017.
1 Like