I know this is a topic that comes up a lot. I have a severe high frequency loss with pretty well preserved low frequencies. I have had several excellent HAs, but occlusion is always a sticking point. Domes are very uncomfortable for me and they occlude. My ears are oddly shaped, so I wear full shell acrylic molds which hold nicely in place. The vents are as large as possible, but the RIC receivers take space away from the ear canal opening. I’m wondering if I go to BTEs with thin tubes, I can have a larger vent. I know that RICs are theoretically better for high frequency loss, but that is offset for me by occlusion problems. Feedback is not a problem. The occasional squeal is fine. --Steve
If I were in your position I would go for a BTE aid and use a thin tube.
You would get better high frequencies if you use a thin tube compared to a ear hook and fat tube.
Phonak’s B90 M is what I wear. If I wear a ear hook and ear mould, I would hear up to 5100hz, if I wear a ear mould with thin tubes, I will hear up to 7100hz so Phonak aids seem better if you wear a thin tube. (Not sure about other manufacturers.)
Sorry, this is backwards.
2 Likes
Please explain. --Steve
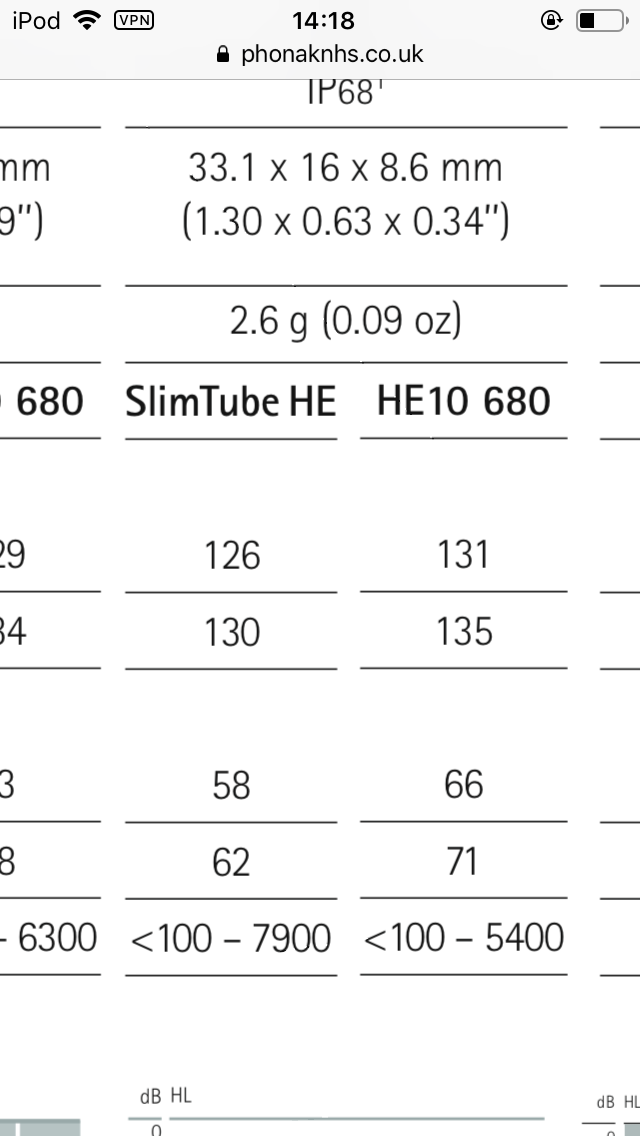
Looking at Phonakpro the Sky M, P and PR BTE aids are either way concerning the frequencies with slimtubes and standard size 13 tubes.
Realistically, given constraints of the sloping loss and feedback management, simring isn’t going hit targets at 6-8 kHz anyway.
But physically, it’s harder to push sound down a slim tube than a thicker tube. Generally, moving from a thick to a thin tube will strangle the highs.
Phonak knows it too. In that same document, look at how the recommended fitting graph changes in the highs for slim vs standard tube. The ear simulator might show a tail out to 7900, but for someone with a sloping loss that’s not going to mean anything.
2 Likes
That is what I was thinking also.
1 Like
The fitting formula takes all this information to make a prescription. So when a person adds their audiogram and acoustics into the hearing aid software it will be obvious if slimtubes would function as needed for a particular hearing loss.
Variances to software input can really mess up a prescription, at least this is what I have seen.
1 Like
This information is really helpful, disappointing but not surprising. So, how can I have my cake and eat it? Can I stay with my RICs and skeleton molds, and also build a maximally sized vent? I have great hearing aids to compensate for my high frequency hearing loss. At the same time, there is no efficient way to let in all the natural low frequencies which I can hear pretty well unaided. --Steve
I’m starting to think our “good bass” is little use. To get LOTS of treble without squeal we need a pretty good seal. Which blocks bass too. And it isn’t really a problem to make the HA do 200hz on up. (Below 100Hz comes in anyway.)
You may indeed be able to get a larger vent with a BTE. Particularly if rather than being super small your ear canal is just very oval/narrow. An earmold is also easier to modify, so if the first fit is occluding you can shorten the vent bit by bit to see if you can get to a good balance of feedback management versus occlusion.
Keep in mind that even at the low frequencies, you don’t have “normal” hearing. You have mild hearing loss. If the problem you are running into is that you feel your ears are plugged up, that you aren’t hearing low frequencies as well as you should, that is not occlusion that we worry about–that can be replaced by cranking up the gain on the hearing aids (and closing the vent). Troublesome occlusion comes as an unpleasantly weird effect on your own voice, even when the hearing aids are in and off. It also comes as uncomfortably loud body noises, such as crunching. Some people with your loss aren’t actually that sensitive to it, and some people are very sensitive to it–it depends on your individual anatomy (and to some degree, your tolerance for things sounding different).
Given your loss, I wouldn’t expect the high frequencies to be impacted negatively with a move to a standard tube BTE. If you stay with a RIC, what is going to work best will again depend on your anatomy. Sometimes a shallow, wide-open skeleton will be better than a dome for feedback, but sometimes a smaller dome will be better if it can be seated more deeply. I would recommend you go with what you are the most comfortable with and work within those parameters to optimize the fit. Some people are more comfortable in BTEs (I have a mild BTE bias because of their robustness and fit) but some people are more comfortable in RICs (i.e. if they are sensitive to BTEs making their ears feel hot or to the weight of the device).
It you’re looking to do some trial and error, there will likely be a non-refundable expense associated with the earmolds. Good quality earmolds are more expensive than they seem like they should be–I run into a lot of sticker shock for earmolds in particular, but our margins there are actually very low.
1 Like
I have tried molds with small vents or no vents. The occlusion effect is terrible. I tried ITEs and had the same problem. When they open the vent, the occlusion gets much better. My current RICS with open molds give me a decent amount of treble.
Even when I turn up the gain, there is only the occasional squeal, especially if I come close to an object or a piece of clothing. I don’t get continuous feedback, and I am not particularly bothered when my hearing aids squeal once in a while. I can usually avoid those situations.
Thank you so much for your thoughtful comments. They are very helpful to me.
I forget that I experience occlusion differently than most.
With any modern aid, steady squeal should not happen. While the algorithms can’t figure out all situations (music especially), generally a steady tone is “wrong” and the digi-processor can phase-cancel it or dial-down overall gain.
1 Like