Yeah @MDB I have no idea how REM is set up, not a scooby ![]() I tend to agree with @tenkan though, REM isn’t the b-all & end all of hearing aid best practices, a good A.uD or a good DIY’er, will probably get a better fit without REM, I have personally seen or in this case heard, a far better setup without REM, but that was from an extremely gifted A.uD… Cheers Kev
I tend to agree with @tenkan though, REM isn’t the b-all & end all of hearing aid best practices, a good A.uD or a good DIY’er, will probably get a better fit without REM, I have personally seen or in this case heard, a far better setup without REM, but that was from an extremely gifted A.uD… Cheers Kev ![]()
Yes. Regardless of the preset you use in the hearing aid software, you can adjust gain to better approximate one set of targets or another. Depending on what all is involved with NAL-NL3, more factors may be at play, but if it is a formula for prescribing gain, then you should be able to just fine tune to it.
2 Likes
You are correct in that not all real ear measurements involve a fitting formula e.g. REUG, RECD, etc. But the purpose of NAL-NL2 the fitting formula in Target/Genie/etc. is to meet NAL-NL2 the prescriptive targets, the approximation of which is verified during real ear (or test box) measurements. So although they are separate components, real ear measurements and a manufacturer’s fitting formula are absolutely related in how they come together during a hearing aid fitting. This is likely not grounds for an argument here, but I figured some clarification would be useful.
Also, clinically we calibrate the measurement equipment (audiometers, probe mics, etc.), but then verify hearing aid function after. Again, probably not grounds for a huge argument.
3 Likes
Chiming in in support: If I set a hearing aid to NL2 and then carefully verify it to DSL, the fitting is DSL, and vice versa. Clinicians generally want to pick the same rationale in the software as they are fitting to using REM because getting from software-NL2 to DSL is much more annoying than getting from software-DSL to DSL and takes up more clinical time.
Rationales are a gain prescription. Unless NL3 has added something unexpected, it will be backwards compatible with everything. I suspect it has used AI to support its development, but will still be a gain prescription.
Additionally, one of the big differences between proprietary targets and independent targets is that the latter come out of research done by academic institutions which are supported by your tax dollars and aren’t as profit driven as private companies that make hearing aids. The independent rationales are also open to other independent research bodies to critique and test, rather than just being some secret manufacturer sauce.
What can we do to demystify the fitting rationale on these boards? Even proprietary targets are all largely based off of NL2 with minor tweaks that, on average, reduce gain to make first fit more acceptable to the user. Here and there manufacturers have done “internal research” and discovered that in their small group people liked 1 dB of extra gain at 2k.
NL2 and DSL have gotten closer over time during their development, which suggests they have been converging on some optimized spot. I would not expect drastic changes in NL3 for most people. What I would love, however, would be refined targets for individual populations that are a bit outside of the average. Reverse slope, for example. Asymmetries.
5 Likes
well this “virtual patient” as being revolutionary … NAH, the first time I saw a patient simulator was call the OTIS, subscription based company lets you learn how to take an audiogram. This was a while ago…
2 Likes
Great to see that there is probably common ground that will be discovered by different approaches (NAL and DSL), which will additionally strengthen the scientific basis of the fitting rationale.
Admittedly, somewhat selfishly, but I’m counting on it! ![]() Maybe it will take a CI into consideration of e.g. loudness balancing, but this will be rather in NAL-NL4…
Maybe it will take a CI into consideration of e.g. loudness balancing, but this will be rather in NAL-NL4…
1 Like
Oh yes, this would be lovely. But one of the barriers to that where I am is that CI clinicians are often not hearing aid clinicians. I still see my CI patients for their hearing aid on the other ear but they go to a bigger centre for CI mapping that is connected to our public health system. It’s nice that I get to see how they are doing, but it feels a bit silly that the CI team doesn’t just fit the hearing aid as well. I think if one was doing both it would be better for seeing and understanding the overall patterns in how patients prefer the two ears to be balanced out. Though in that case there is also so much neural adaptation that you probably don’t really know what is going to be your end spot until a few years in.
4 Likes
It’s also possible NAL and DSL made similar initial assumptions. Convergence may or may not be good. Those assumptions were made when the available technology and compute was very different. Not everyone wants aids so focused on human speech versus the broader range of sounds.
1 Like
New presentation about NAL-NL3 from NAL director:
(the PDF is 7.25 MB, but the app won’t let me upload it, despite a 10.7 MB limit. @AbramBaileyAuD, perhaps you could check this.)
Source:
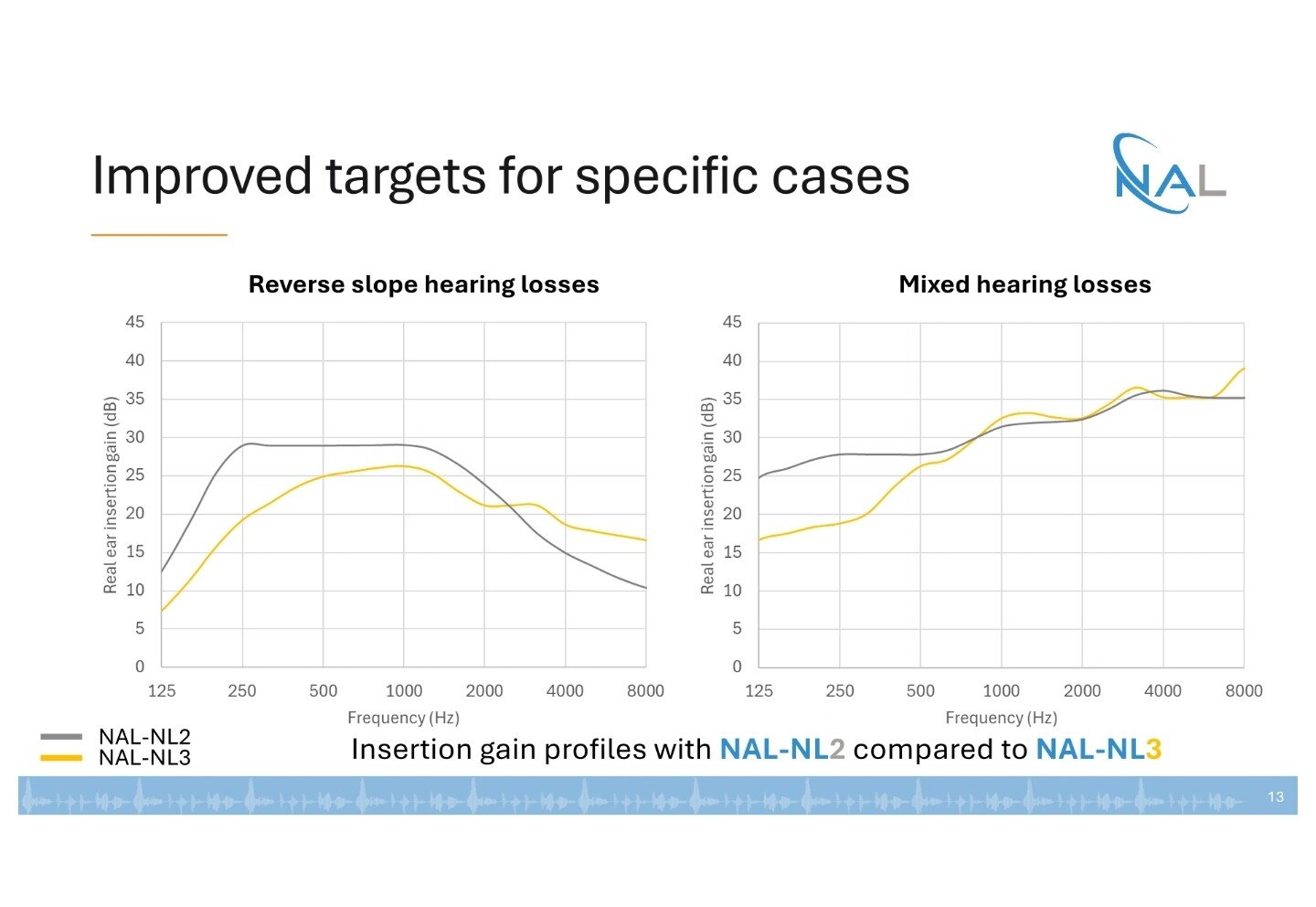
I’d be happy with the assessment that for reverse slope losses NAL 2 was off. The changes for mixed losses are a bit obvious in respect of occlusion effects too.
1 Like
One question: is there any hidden thing that those paradigms do beside changing the fitting?
I mean, if I reproduce with DSL the same fitting that NAL2 suggests, will the HAs sound the same across the two paradigms?
1 Like
Probably MPOs (DSL 5.0 takes UCLs into account, NAL-NL2 not). I don’t know what about attack and release time.
However, if we assume a ±5 dB acceptable deviation and do not consider targets above 4000 Hz, DSL 5.0 and NAL-NL2 might look very similar.
You don’t make one prescription ‘from’ another: you stuff your figures into the system, the formula derives a target by applying the prescription formula at each frequency and then you tune your hearing aid output to meet the desired levels of gain/output based on a given input with REM.
The original ’position’ becomes completely overwritten by the new gain levels, set to achieve the expected results. ULLs will usually default to around 105/110dB within the aid unless there’s either a big conductive element or in the case of more severe losses.
The manufacturer’s target becomes redundant once you’ve done the REM as there’s no proper compensation for canal volume/impedance/venting. The NAL 2/3 target just gets painted across the REM screen so you can tell if the aid is actually doing its thing or not.
1 Like
Thankyou for posting that it was a good read.
My 2010 iMac stopped working because Apple stopped upgrading it.
I bought a new iMac a year ago. Wish I hadn’t.