Will be going in to Costco to get my KS8 HA’s fitted this coming week and I am trying to get up to speed on how they will do the fitting. I have watched the video by Doctor Cliff on REM and he seems to focus on two important points.
Manufacturers assume many HA dispensers will not do REM and as a result they provide a manufacturer specific fitting process which is conservative at the higher frequencies compared to the industry standard NAL-NL2 fit to ensure patients will not complain. i.e. better to have less amplification than too much. A quick and dirty, but safe approach.
REM is best practice because there will be a difference between what the software expects to get for HA amplitudes in the ear and the individual ear specific results. The REM process should be used to correct for these differences.
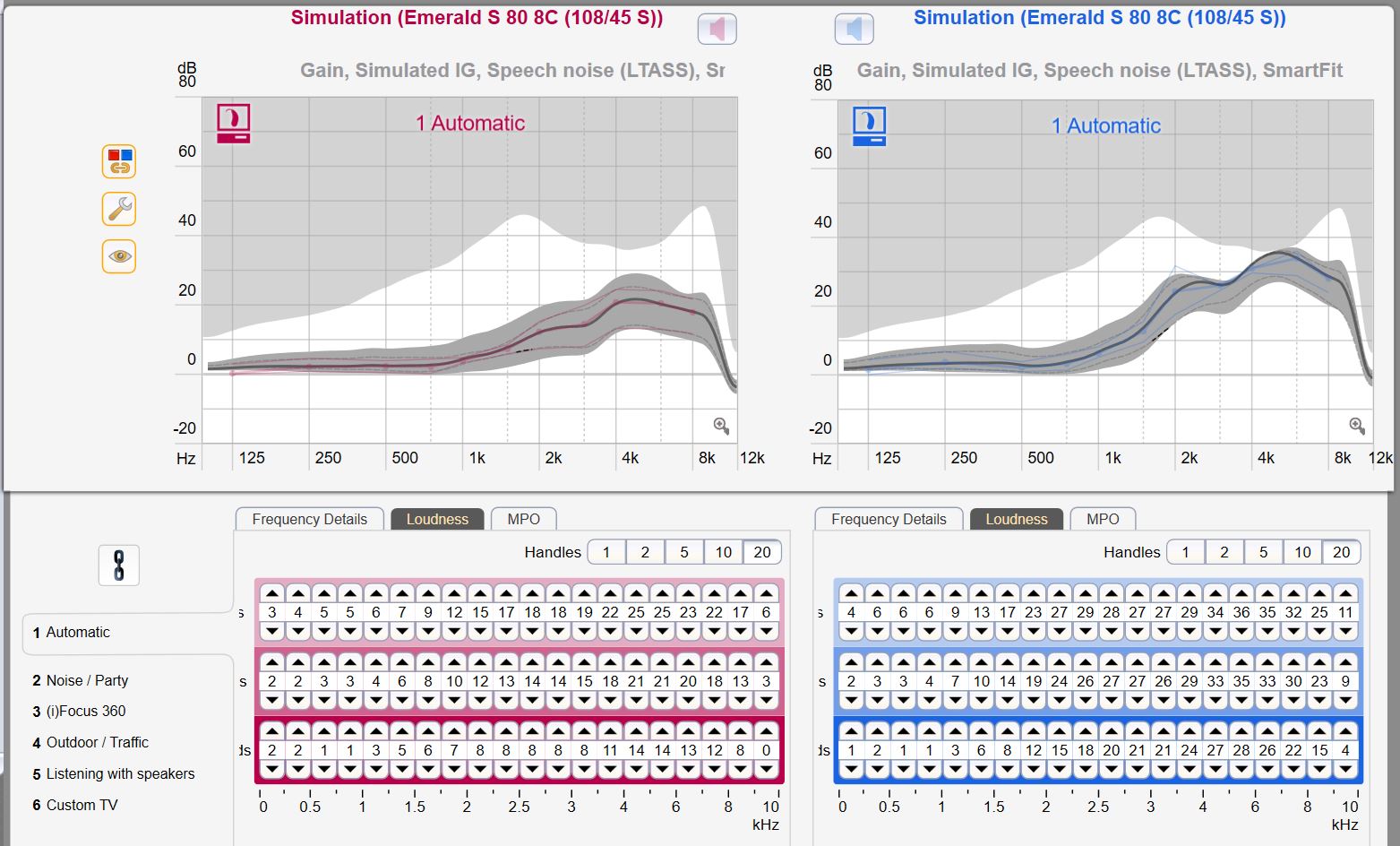
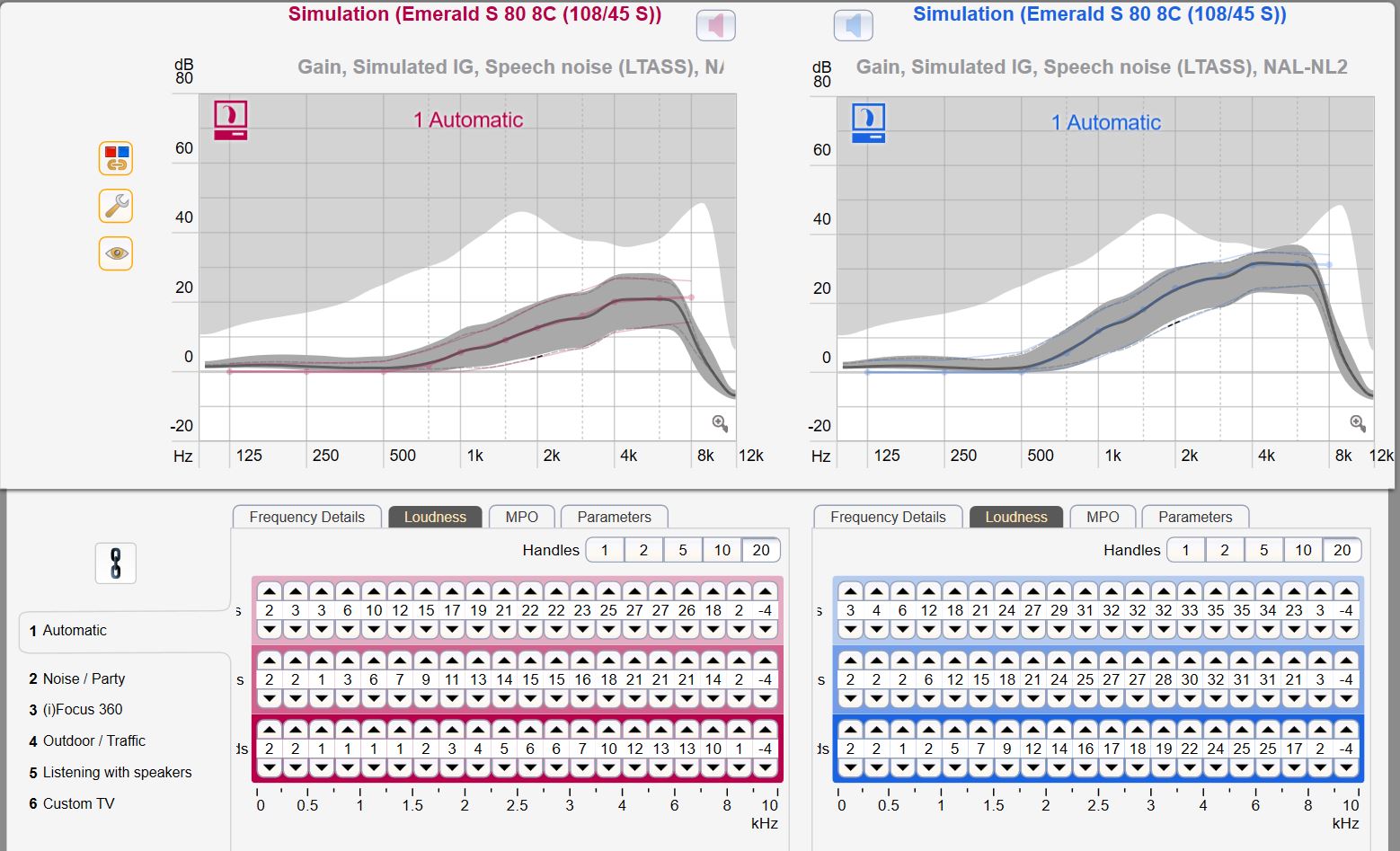
This makes perfect sense to me. I have downloaded the Connexx 8 software and entered my specific audiogram data that I got from the first appointment at Costco. I then went through both the NAL-NL2 and the SmartFit (Rexton) method. The screen shot for each method is shown below, with the Soft, Medium, Loud loudness settings showing. I am understanding this to be the gain after the applied compression process. I notice two difference in the methods:
The target correction for the NAL-NL2 method contrary to what Doctor Cliff says is lower than the SmartFit manufacturer target especially at the higher frequencies.
The gain seems to truncate and drop off suddenly for the NAL-NL2 at the very high frequencies above 8 kHz, while the SmartFit continues to apply correction and gain up to the 10 kHz bandwidth of the KS8 HA’s.
As a result my thoughts are that the SmartFit process sets the better target level, and when corrected with the REM it would be the best method to use. Would I be correct in that assumption? Comments?
The two screenshots with the SmartFit first and the NAL-NL2 one second:
The target for REM that the Costco providers I’ve seen has been NAL-NL2 (even though they used SmartFit to do the fitting). However, my experience is that they tend to aim for within 10dB, so they’re not very precise. I assume those curves are with “New user” instead of “Experienced?”
Unless I messed up, the data in both cases is for Experienced, not New User. The technician at Costco indicated she goes for the full correction at first fit.
You can see the fitting method for each set just above the graph for the left ear, so I don’t think the are mixed up. The top set of graphs are the SmartFit ones. What I am seeing is more gain for the SmartFit, and more compression (less difference between moderate and loud) for the SmartFit.
Am I going to be asking for too much to request the REM be adjusted to the SmartFit target values, and to be closer than 10 dB for error? 10 dB is a lot to be off, especially if it is too high…
As a thought from a while ago…I would suggest just going in there and let them do their thing and them sending you off into the world.
There will be followups of course. Increase your wishes then and they’ll see that you’ve done your homework.
I don’t think you can do REM to SmartFit. I agree with Z10 to just see how it goes initially. Certainly fine to ask questions why they are doing things a certain way.
MDB is correct that REM cannot be done to SmartFit targets. Those targets are proprietary; we do not know what they are. NAL/DSL targets are independent; they have been developed/tested/refined by academic institutions and that information is public (well, in some cases behind a journal paywall). Presumably, proprietary targets have had some sort of market research done to determine that they are useful, but we have no idea what that might have been. Most of them are at least based off of NAL-NL1 or NL2 these days I think. One would imagine that deviations from those targets have been made because the manufacturers have determined benefits? Although I suppose they may also have been made because some group of engineers thought it seemed like a good idea. Also, “more gain” is not necessarily the general marker of “better”.
Keep in mind, too, that targets are external to the hearing aid. The software might suggest that the hearing aid is doing something, but unless it is measured on the ear you don’t precisely know what it is doing. On the one hand, as you say, when the software claims that it is fit to NAL-NL2 targets it is often not (although the deviation has come down since some of those old studies). On the other hand, hearing aid output is affected by ear canal acoustics (and coupling) which are different from person to person.
You are not asking too much. The goal for pediatric fittings, for example, which are a bit more standardized and constrained than adults fittings, are less the 5 dB RMS error and we regularly attain less than 2 dB, particularly when we aren’t running up against the limits of the device or of loudness tolerance.
It goes through the fitting process in quite some detail. I am using Rexton Connexx Eight software in the simulation mode, and this document based on the Signia Connexx Eight. The terminology needs some translation between Rexton and Signia terms, but as far as I can see the software is identical. The generic fitting formulas like NAL-NL2 are the same, but Signia calls the proprietary formula Nx-Fit, while Rexton calls it SmartFit.
In the First Fit process you select the Fitting Formula, and I can see no reason why you cannot use the proprietary method. It generates the target setting curve. Next when the REM equipment is connected, another selection box displays in the bottom right of the screen which Signia calls AutoFit. Confused yet? Since I have no REM equipment connected it does not show up on my screen and I don’t know for sure what Rexton calls it, but it may be AutoFit as well.
This is where the auto fitting process starts and gains are set automatically to the already selected Fitting Formula. I know that the Costco center I went to uses the Otometrics Aurical system, and their site says it is compatible with Connexx Eight (Ver 8.5) using AutoFit. A quote from the article:
"Before starting the AutoFit procedure, the desired prescription formula and user experience level should be selected. There is a choice of 1/3 gain, NAL-NL1, NAL-NL2, DSL-v5 and proprietary fitting formula as e.g. Nx-Fit [see Figure 4]."
So I am thinking that there is no reason they cannot use the Reston SmartFit formula for the REM target. My plan is to ask them what method they use and why, and then go from there. If it is an arbitrary decision on their part then I will ask for the SmartFit. If they never use it and don’t know how, then I guess I will have to go with the flow.
Stupid question here. I presume Rexton SmartFit is different from ReSound Smart Fit 1.3 due to different companies. ReSound Smart Fit, I believe, from just skimming over their AutoRem course materials can interface with REM software/hardware from three different companies and incorporate the REM measurements directly into the fit. The one thing that I noticed about their marketing claims for this, is they claimed it saved the provider several minutes of time on each fit- which didn’t seem like a particularly big deal to me but perhaps it adds up over a day or over the course of a patient requesting many fitting changes over time. So Rexton SmartFit is different, cannot interface with REM instruments/software directly, and the REM measurements cannot otherwise be easily sucked up into the fit?
Heh. The irony for us is that we are busy enough that those minutes would make a difference, but so busy that we haven’t yet had time to experiment with the autofit to see if it works well.
But in terms of incorporating into the fit–REM adjustments are always incorporated into the fit but in one case the clinician adjusts by hand and in the other the software can do it. Or, I’m not sure what you are imagining?
I have no idea what the Rexton can do. Costco software is only slightly different in some odd ways, from what I’ve seen, but it’s possible they knocked that feature out for Costco. It actually sounds like something that Costco would probably want. Costco Canada, anyway, which has a very clever woman running lead to ensure a fairly high, standardized quality of care. I don’t think Costco US has an American counterpart to match her.
As an aside, sometimes when you are running REM in a busy clinic you’ll see something funny that you decide to ignore because you know it’s an artifact. You know what effects are caused by the probe tube being pinched a bit by a tight dome fit, or there was some wax in the way in that ear which make proper placement difficult, etc., and if everything else is looking good and sounding good you might ignore it and move on because you are confident that it is not a true reflection of what the hearing aid output at the eadrum is. The autofit wouldn’t be able to do this I don’t think. I expect it would run a wonky correction around the problem and you might end up having to re-correct that anyway. So also, if you are watching your provider run REM and think something looks a little wiggly on one side, go ahead and ask why they ignored that rather than assuming they are messing things up.
Because the smartfit targets are not in the REM equipment–REM equipment is independent from the manufacturers and the makers of the equipment are not given the proprietary targets, nor are we so we cannot calculate them for your loss and input them into the equipment. You can certainly set the software to smartfit and then verify against NAL (NL1, NL2, whatever the manufacturer suggests is closest) if you wish to, and clinicians will do this for various reasons. What you cannot do is say “I want to make sure that this smartfit software is providing correct gain at the eardrum based on smartfit prescription targets” because outside of manufacturer closed doors those targets essentially do not exist.
The big difference, to me, between independent and proprietary targets is that one is based on verifiable scientific methods that seek to determine an optimal gain prescription and the other could be scientific or could be complete woo and I have no way of knowing. Realistically, they are close. The manufacturers aren’t re-inventing the wheel with their gain prescriptions and they ARE trying to run their research appropriately even though they are not subject to peer-review. They want their product to work the best. Idealistically, I prefer the independent prescriptions.
I am understanding from the way you are approaching this that you are using the REM hardware and software to do the REM? My understanding of the Connex Eight software approach is that you “plug in” the REM equipment and the Connex Eight software uses the measurements from the REM (Otometrics Auricle in Costco’s case). From the article I posted above, it seems the Connex Eight is in control and the REM is the slave equipment providing the REM data using IMC2 data exchange. I can see how the screens change to show this fitting option from the article. The REM target is selected in Connex so of course it knows what it is, even if it is Connex Rexton proprietary.
I guess it comes down to how Costco does it. is the Otometrics Auricle doing the fitting to target, or is the Connex Eight doing it… I suspect which ever way they are doing it, they are not going to change it for me, and I will be stuck with their standard process. AutoFit may be faster, but probably not until they have done it many times and learned how to do it efficiently.
I wish I would have known about this complication before I booked my appointment with this Costco. Perhaps there are different methods used at different Costcos…
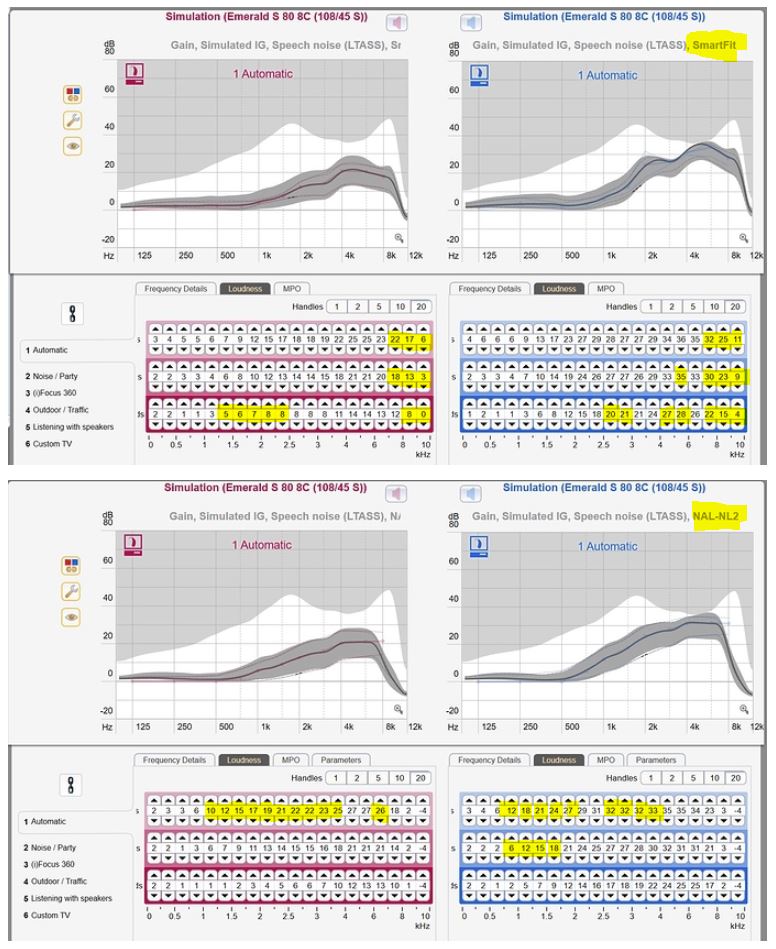
The top set of data is for the SmartFit, and the bottom set is for NAL-NL2. What I am seeing for the right ear at the soft levels at 2k, which is the bottom row of numbers in each set is:
SmartFit - 7-8
NAL-NL2 - 3-4
It seems the SmartFit is boosting the low level more at 2 kHz which to me suggests more compression.
Thinking about this a bit more I guess it will come down to what workflow this specific Costco uses, if it is not standardized across Canada. From what I can see they can use the Otometrics Aurical software as the hub and do REM from there. They claim they are compatible with:
Phonak Target
ReSound Aventa and Smart Fit
Beltone Solus Pro and Solus Max
Oticon Genie and Genie 2
Bernafon Oasisnxt
Sonic EXPRESSfit Pro
Signia Connexx Eight (v. 8.5) using AutoFit
Costco here fits Kirkland (Rexton), Rexton, ReSound, and Phonak, so it may simpler for them to make the Aurical the hub for REM. But at the end of the day I suspect they still have to use each manufacturer’s software to program the HA, so not clear. I will find out when I go I guess…
I rethought this issue a bit, and did some more comparisons on the Loudness charts between SmartFit and NAL-NL2. It seems that the main difference is that the NAL-NL2 boosts the gain in the lower frequencies and in particular in the 1-1.5 kHz range. I highlighted the points where one method or the other gave a gain of 3 dB or more, which is kind of the minimum one can hear. The results:
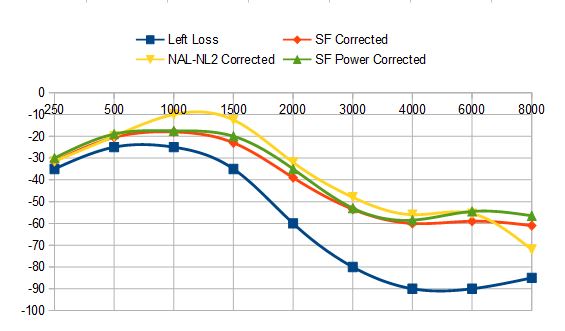
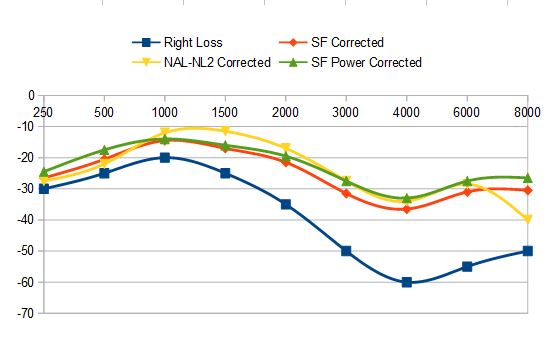
I could not make a lot of sense of this so next I just plotted the gains of each method on the same chart as my Audiogram hearing loss. Probably breaking all kinds of audiology rules by doing that, but I did it anyway. And I found another Fitting target in the process called SmartFit Power, which seems to be one level more aggressive the SmartFit Experienced. It tends to be lower however than NAL-NL2 except at high frequencies. Here is what I got:
I am coming to the conclusion that this correction process with HA’s is pretty crude. The emphasis of the NAL-N2 formula seems to be heavily weighted on emphasizing the midrange frequencies, kind of like a pubic address sound system. Certainly not what one looks for in a high fidelity playback system, but I guess those are the frequencies important to speech.
This may all be a moot point anyway as I may not get any choice in the correction method. If I do, I am leaning toward the SmartFit Power formula. It seems to be the most linear of the available choices.