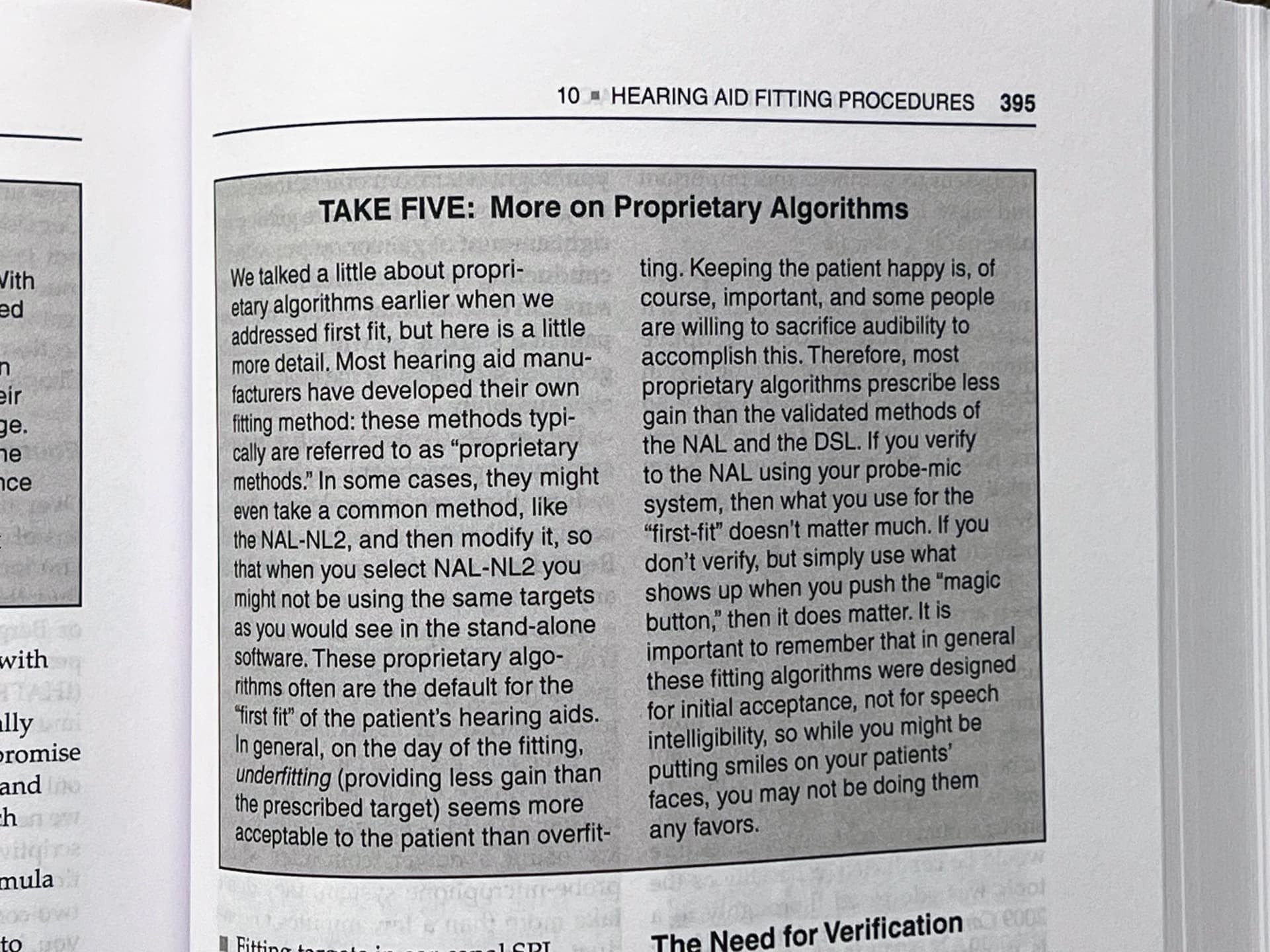
If you take their word for it. The authors of Fitting and Dispensing Hearing Aids Third Edition don’t agree. In particular, see the last sentence in the excerpt below. My audiologist confirmed this when she was fitting my Reals. At least one of the professionals on this forum has posted to the same effect.
5 Likes
I think this discussion has been hashed out before. HCPs seem to take the view that proprietary rationales are used by HA mfgs to “dupe” their users into a comfortable first fit so that they can sell their aids more easily. This is the gist of this source that you’re citing. You can take this book’s word for it, but I won’t.
I think part of the reason why many clinicians take this stance is because the external REM equipment that they have cannot fit to the mfg’s proprietary targets because they’re proprietary, and their REM equipment can only fit to non-proprietary standard fitting rationale targets. Therefore, this is the stance developed, that the standard fitting rationales are THE best, or at least always better than the “underfitting/under performing” proprietary rationales.
I think it’s OK to take that position, but to take it a step further and say that HA mfgs come up with proprietary rationales just to dupe customers into buying their hearing aids more easily on purpose by underfitting it to favor comfort, therefore doing their customers a disservice for the mfg’s own sales gain, is kind of a low road they don’t need to take.
I know that if I use the Oticon VAC+ fitting rationale, there are features in Genie 2 that are available to me, like the Sound Controls features for Brightness perception (from Fuller to Brighter), and for Soft Sound Perception (from Comfort to Detail), that would not be available to me if I go to a program where I select any of the standard fitting rationale. With a program using a standard rationale, the Sound Controls page is grayed out, meaning that I can no longer have the options to use these features.
For clinicians in your book who say that proprietary mfg fitting rationales cannot measure up to the standard fitting rationales because it’s designed for comfort and not speech, I say that I can set the Brightness Perception parameter in the available-only-with VAC+ Sound Controls option to maximum Brighter, and I can probably get the Brightness I need for speech without the need to necessarily resort to NAL-NL2 to get that for me. So it’s not like only NAL-NL2 has the monopoly on brightness necessary for speech. It can be done just the same with a proprietary fitting rationale, as long as your clinician really knows what they’re doing with that mfg’s aids, and is not too busy putting down proprietary fitting rationales instead.
To boost, by using VAC+, I can take advantage of the Oticon Soft Speech Booster feature by setting my Soft Sound Perception value to the max Detail value, something that would not be available if I were to use NAL-NL2 because this is a VAC+ proprietary feature only. If I had favored a standard rationale over VAC+, I would be foregoing a special Oticon-only feature for boosting soft speech that’s to me personally is a very desirable feature.
Below is the link where Oticon talks about their proprietary VAC+ fitting rationale and one of the reasons why they have this VAC+ rationale is to make available something they specifically developed for their VAC+ rationale called the Soft Speech Booster, which can be managed by the Soft Sound Perception parameter mentioned above.
Inium Sense - Soft Speech Booster technology | Oticon.
The Oticon VAC+ rationale was also developed by Oticon to have their own tweaks added in for what they think is a more realistic and better approach for cookie bite fitting based on their own research. I remember reading a whole presentation from Donald Schum about this from Audiology Online. We have some members of this forum who have cookie bite hearing loss ( @Abarsanti is one whom I remember) who sought out to try VAC+ and seemed to have a positive experience from it.
The Oticon whitepaper in the link below titled “The REM Cookbook” says that one of the advantages of the REM Autofit feature in their Genie 2 software is the ability to select VAC+ as the target fitting rationale to verify against if desired, which is not possible when using an external REM setup because external REM setups don’t have access to the proprietary VAC+ rationale.
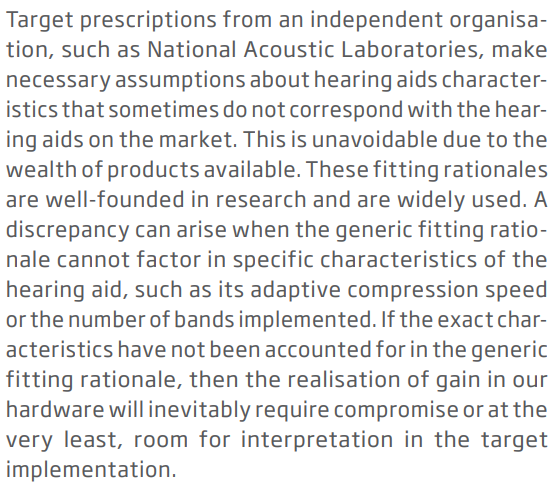
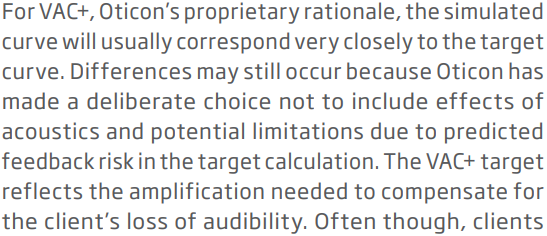
Furthermore, another Oticon whitepaper titled “Client Target and REMs” (see link below) on page 3 says that standard generic fitting rationales need to make necessary assumptions about certain characteristics that sometimes do not correspond to the actual HAs available on the market, which can lead to discrepancies when the generic rationale cannot factor in specific characteristics that the hearing aid has (like the adaptive compression speed, or the number of bands the HA has). Due to this, the realization of gain in the HA can be compromised. There seems to be deliberate choices that Oticon made and put in, or not put in, to their VAC+ rationale that are not necessarily reflected and included in the standard generic fitting rationales.
I’ve cut and pasted the exact wordings for this in the screenshots below if somebody wants to read it in more details.
One final personal note I have on this. As an Oticon wearer, I actually have a program with VAC+ (my default program), a program for music, then I also have a program for NAL_NL2, and a program for DSL v5,0 Adult (both of which are standard rationales). I’ve tried them all and in the end, for 90% or my use, I still prefer the program with VAC+ the most. It’s not because I like the “comfort” it gives, but it’s because it sounds the most natural overall to me, and not as harsh as the standard fitting rationales. And I still get plenty of brightness from it to understand speech just fine, because I have the (exclusively available only in VAC+) Brightness Perception parameter that VAC+ gives me to select.
7 Likes
“My” book was written by these guys:
You really think that reading Oticon’s external marketing and professional literature qualifies you to argue with them about how the hearing aid industry works? And they didn’t use the word “dupe,” you did.
1 Like
I really think that they’re entitled to their opinions, but they’re not the only qualified professionals in the field. And I think that they’re just making a very sweeping generalization and they’re putting the same hat on everybody. It’s like saying “lawyers are scumbags” and “car dealers are scam artists”.
And I didn’t quote any external Oticon’s marketing materials here like you said because marketing materials never go into this level of details anway. I quoted 2 sources of professional literature and 1 source of a presentation from Audiology Online, all meant for HCPs as the audience, not meant for consumers.
So while these professional sources I quote still don’t qualify me to argue with your well credentialed book authors (like you said), in the same vein, that same book that you quoted me doesn’t qualify you to argue against the 3 professional literatures I quoted back either. I never tried to argue with your book authors anyway. I’m just arguing with you. You quoted your book source, and I quoted my professional literature sources back, just to show that not everything is black and white and one sided.
The bottom line is that it’s easy to make generalization about proprietary fitting rationales like what the book does, but my argument is that it’s not that simple. I believe that there are a lot more reasons why HA mfgs spend the money and effort to come up with their own proprietary fitting rationales, more than simply just to make sure that the first initial fit is comfortable to keep their clients happy. So I think in that sense, the book presented a lopsided view which I don’t agree with. And to elaborate on why I don’t agree with that lopsided view, I cited you a bunch of reasons specific to Oticon based on their professional literature.
2 Likes
Do you disagree that most proprietary algorithms prescribe less gain than standard fitting rationales? Or do you disagree that proprietary algorithms were designed that way? Or, what in that book excerpt do you disagree with?
How do you know that your hearing is dropped? Do you often go for an audiometric hearing test? May I ask, do you do IN-situ?
What I don’t agree with is their conclusion in their last sentence that proprietary algorithms are designed for initial acceptance, not for speech intelligibility. YOU yourself, told me to look at that particular last sentence there, too, no?
What does that imply? That HA mfgs create proprietary algorithms SOLELY for the purpose of initial acceptance? Which implies happy customers (also mentioned by the book), which implies closing the sale, no return after trial (not mentioned by the book, just deduced by me). But it’s obvious that the book is saying that the HA mfg’s proprietaries are no good for speech compared to standard algorithms. It’s also implying that HA mfg’s don’t have the customer’s interest at heart because they just want to fool the customer into initial acceptance by keeping them happy with it by this design, and if the HCP fits them with proprietary algorithms, then it would be a disservice to the customers (the book says “not doing them any favors” → same thing, different words).
The take-away from this section you refered to is obvious, and I’m sure you brought it up to expound on the same point, too → Proprietary algorithms → Bad for speech → designed ONLY to keep the customer happy for initial acceptance → Standard algorithms → best for speech.
So I proceeded to debunk this implication by:
-
Showing how a proprietary algorithm like VAC+ was done for their special exclusive Oticon only feature → Soft Speech Booster.
-
Has other Oticon only features as well that gives more flexibility like Brightness perception. If the client uses VAC+ and wants the sound to be brighter, like how the standard rationales are bright to begin with, then they can simply adjust this slider to Brighter. It’s not like they’re doomed with VAC+ to be duller forever, and therefore always inferior to standard rationales.
-
But if they find it too bright and they like it to be fuller because they don’t need it to be too bright to understand speech, then at least they are given that flexibility to make it fuller and less bright. But if they use a standard rationale, they’re stuck with the brightness for good, unless the HCP has to go into Fine Tuning and make it less bright, which is a lot more work than sliding a slider a couple of notches to the left.
-
The whole point of 1, 2 and 3 above speaks to the flexibility for customization on VAC+, which would not be available if a standard rationale is used. So proprietary rationales don’t underfit, and are not designed to underfit like you and the book are telling people. At least for VAC+, they’re designed to give you the full spectrum from warmer to brighter. You can make them underfit, or you can make them just right, or you can make them overfit, all at the touch of a simple slider. At least you have 3 options there (or anything in between). You only have 1 option for standard rationale, just AS IS, no easy change, no easy adjustment.
-
Oh wait, there’s more. VAC+ is designed to work better for people with cookie bite losses, according to the research from Oticon. I don’t know enough about how well the standard rationales work for cookie bite losses so I won’t comment further than this.
-
Oh wait, there’s more. Standard rationales have to make assumptions about how the specific HAs work, between all the various brands and models. Proprietary rationales know EXACTLY how their own HA brand/models work, and they build their own rationales around that. No assumptions that may prove to be incorrect is to be contended with.
The bottom line is that the book is making a very far-fetched and overly simplistic generalization that proprietary are inflexible algorithms that are designed almost exclusively to underfit just for the purpose of happy initial acceptance to begin with, and cannot be changed, and should not be used in place of standard rationales, because they’re not good for speech at all. I totally disagree with this.
I think proprietary rationales afford the mfg to put in a lot of adjustability and built-in accuracies that are synergistic with the specific hearing aids’ design features and the mfg’s intended philosophy, none of which can be done to a fixed and rigid standard rationale that can’t be modified. Remember, HA mfgs simply can’t mess around with standard rationales to improve things like they can with their own proprietary rationales, because standards are fixed and you don’t/can’t mess with them. HA mfgs come up with their own proprietary rationales so that they can have better control over them for accuracy and adjustability and flexibility, not for happy initial acceptance.
4 Likes
I can’t hear as well and was warned my medical treatment can cause further hearing loss.
The audiologist/hospital tested me and new hearing aids issued.
I haven’t done a In-Situ since hearing dropped but I have in the past.
1 Like
Completely agree @Volusiano . If it was just about initial acceptance why would they bother looking any further than their acceptance/acclimatisation level formulae.
When you input client info into the software it will ask whether they are a new/experienced user and basically program to 80-100% of the target. It’s quite clear that it’s a shaped adjustment too for comfort. A few years ago Phonak reconfigured their ‘first fit’ approach to make it more aggressive - to help first time users accept aids with comfortable sound (which is actually really important to start with) but they wouldn’t be doing this if that was the point of their own fitting formulae.
In addition Phonak offer an ‘slow compression’ fitting formula specifically for some users with severe/profound losses. It’s based on research that 50% s/p users prefer this. There’s no difference in the amplification compared to the fast compression version. It just adds to the idea that manufacturers really are working with the best intentions for hearing aid users.
2 Likes
Let me try to keep the question a practical one. This is a textbook for students who are going to dispense hearing aids. Once on the job, they’re going to fit aids to clients who’ve never worn aids before, and send them out the door to get used to them, with little or no on-the-spot tweaking on top of the first fit (excluding possible REM which changes everything).
The authors are saying that doing the first fit with a standard rationale rather than a proprietary one will provide better speech intelligibility right off the bat, and therefore serve the client better. Do you think this is good advice for hearing-aid-dispensers-to-be?
Incidentally, I think the authors are distinguished by virtue of being well-connected, not just well-credentialed. The top executives at William Demant or Sonova or whatever would probably pick up the phone if they called.
1 Like
I think it’s outdated. In the case of WS Audiology (Signias, Rextons…) their AXFit/IXFit algo, is heavily tied to their automatic/“smart” features, which are increasing with each generation.
Upon initial fit they will perform “profile setup”, which based on user experience wiill apply certain amount of prescribed gain (amongst other things) independently from algo.
To my hearing loss, VAC+ prescribes higher targets than NAL-NL2 and DSAL v5, and about the same as NAL-NL1.
Well connected and well credential professionals are not infallible and not necessarily good teachers either. Even if they were good teachers, they could also have bad teaching moments. I think this special highlighted section in their book to single out proprietary rationales as not being appropriate for speech but only designed for initial happy acceptance is a bad teaching moment.
I think what they said in that section is not good advice. They’re telling their students (the beginning practitioners) to simply forgo proprietary rationales altogether right off the bat and just stick with standard rationales in the name of speech. This is bad advice because
-
their premise that proprietary rationales can never be as good as standard rationales when it comes to speech clarity no matter what is not true.
-
They’re also totally ignoring the advantages of proprietary rationales (which standard fitting rationales simply can’t have because they’re standard and locked out) that they should be teaching their students about but they don’t.
-
They make it sound as if the first fit is the only fit, and the practitioner will never see the client again for subsequent adjustments after the first fit, so the practitioner better focus on speech right away, because whatever they do on this first fit will be set in stone forever. There’s nothing wrong with doing the first fit for comfort for happy initial acceptance, and on subsequent visit, if the client complains that they’re not hearing speech well, then either tweak the proprietary rationale for speech clarity, or add the standard rationales in and ask the client to try them all out and compare against the proprietary rationale.
Actually, the first fit usually will/should involve REM to begin with. The question then is whether to choose the prescribed gain to be a proprietary-based or to be a standard-based rationale. Then the next question is whether to choose the target gain to be proprietary-based or the standard-based rationale. Usually, the only time the target gain can be proprietary based is if REM is done in conjunction with the HA mfg’s software, because only the HA mfg’s software would know how to calculate a target that is based on a proprietary rationale anyway. If stand-alone third party REM equipment and software are used, then there’s really no choice but to set the target gain to be standard-based, because the external software does not have the proprietary knowledge to compute a proprietary-based target anyway.
So if the prescribed gain is chosen to be derived from the proprietary rationale, but external software is used, then the REM adjustment will use the standard-rationale based target gain anyway, so that the end result will “sound” like the standard rationale sound. In this scenario, what’s the problem that the book authors are pointing out anyway? There’s no problem. This is probably the most common scenario that usually happens in my opinion.
On the other hand, if the prescribed gain is chosen to be derived from the proprietary rationale, AND the internal HA mfg’s software is used, then the target gain can be calculated to be based on the proprietary rationale as well. Here, BOTH prescribed gain and target gain are proprietary based. So are the book authors saying that even if REM is done here to match with the target gain curve, this target gain curve is no good for speech compared to a standard-rationale based target gain curve? This is where I disagree. The clinician would be doing the client NO disservice here because the clinician is doing everything by the book (not by the authors’ book apparently, lol).
Granted, even if it were true that after matching the proprietary target gain curve and sending the client off, the client WILL eventually come back after the initial fitting for adjustment, and if it’s not up to snuff for speech, then the client will complain, and the clinician will adjust further until the client is happy. That’s the process anyway regardless of which kind of rationale is used, no?
I have strong reasons to believe that as long as the clinician knows what they’re doing, and they keep making adjustment for speech on subsequent visits from the client, regardless of whether the rationale chosen is proprietary or standard, one rationale will not always be inferior or superior to the other when it comes to speech clarity, and either rationale types can be adjusted to improve speech clarity.
The book’s authors seem to make it all about choosing the right rationale (the standard ones) and avoiding the wrong rationale (the proprietary ones) right up front in the name of speech clarity. I just don’t agree with this. So I don’t think that this section of the book gave good advice to the students specific to that topic.
5 Likes
Are you really shrugging off the difficulties experienced by the mass of hearing aid buyers who aren’t DIY’ers, or just flailing around while trying to dig in your heels and not admit you’re wrong? Besides, what do you even know about non-Oticon fitting rationales, other than marketing materials and white papers? Whatever, I give up on trying to convince you. Of course, if I come across you spewing this misinformation in the future, to the detriment of innocent users, I’ll feel an obligation to correct you and refer to this thread.
Now come on guys, please play nicely!
It’s interesting to read what you are writing but not when you start getting cross with each other!
2 Likes
Did you see any mention by me about DYI’er in my posts around this discussion? Even on what you quoted me above, I only talked about the client coming back to see the clinician for further adjustments. Or are you saying that the mass of hearing aid buyers only have 1 chance of fitting and cannot come back for subsequent adjustments by their HCP, like the book implies?
The exchanges so far has been civil enough, you kept asking me probing questions, and I gave you my answers. Unfortunately my answers are not what you want to hear. But it’s looking like you’re getting hot headed here, so I’m going to take the high road and refrain from snapping back.
Also, we should give the readers enough credit that they will be able to sort out what they read and judge for themselves what they want to believe. Nobody is trying to fool anybody here. Everyone are just expressing their opinions on this forum, and disagreement will come. Readers on this forum are smart enough to fend for themselves and are not innocent victims who need to be protected.
6 Likes
Then how to solve the problem of underfitting when using the proprietary rationale? It does happen. And I personally have had such experiences on at least three fittings.
The solution to resolve underfitting to any rationale is to do REM, period. The question is which fitting rationale target to adjust to in REM. If REM is done using stand-alone equipment and software, then no proprietary fitting formula target can be generated to match against because the formula is proprietary and not available to calculate the target. So even if the prescription is to a proprietary fitting rationale, the clinician will only be able to use just a calculated standard fitting rationale target (like NAL-NL2 for example) to adjust REM to.
Then what you end up having is a prescribed proprietary fitting rationale that ends up sounding like the standard fitting rationale target that it’s been adjusted to. But at least now, it’s still “operated” using a VAC+ prescription. Any adjustment option that’s only exclusively available if the proprietary fitting rationale is prescribed is now available for use. Also, gains calculated by the hearing aids for various listening situations are actually calculated using the proprietary fitting formula. Compression ratios used will also be based on the proprietary fitting formula, for example.
Usually, the only way to be able to calculate a REM target that’s based on the proprietary fitting formula is to run REM using the software of the HA mfg that has information about their proprietary fitting formula in order to know how to calculate it properly. For example, with Oticon Genie 2, it has a feature called REM Autofit that can be used with a compatible REM hardware equipment (like Verifit for example), whereby Genie 2 will automatically do REM adjustment for the clinician against its own calculated proprietary VAC+ target. Only then will the final REM adjusted result sounds like a VAC+ formula and not sound like another standard formula that would have been used by a stand-alone REM software.
1 Like
One would think that standalone equipment would be able to accept a list of calculated targets. But maybe not, for some reason.
Excellent point there. I’m not sure if an automation setup is already available to do this because HA mfgs may be resistant to cooperate and want insist on or promote doing REM with compatible REM equipment using their own software (like the REM Autofit in Oticon Genie 2).
But I would think that if the clinician is willing to go through the manual process of capturing the calculated target for the proprietary formula and enter it into the third party REM software somehow, then do REM adjustment against it, that’s definitely possible. The question is how many clinician would want to bother with it because it requires more time than they’re willing to put in, unless specifically requested by the client. And most of the times, the client doesn’t know any better to make such a request in the first place.