Something I noticed yesterday: when I hum I hear no distortion and the frequency response is perfectly even across both ears, right down to the lowest note I can hum, which is fairly low since I’m a baritone/tenor.
If it was sensorineural hearing loss that should also apply to the sound of my own voice, no? In which case the lowest notes would be in my “good” ear only?
I have an ENT appointment in a week and I’m thinking it would be good to do some more testing there.
It could be some weirdy form of otosclerosis, but; there’s no Carhart Notch and the asymmetrical nature would indicate otherwise.
I’d go with a loss of cochlear function, which could indicate calcification of the deeper parts of the cochlear (again Asym?). Dead(ish)region of the basilar membrane or fluid loss to the innermost part of the cochlear.
Have you been bashed on that side of the head?; Perlilymph fistula occurs when the leverage of the mass of the ossicles tears a gap in the tissue at the footplate of the stapes.
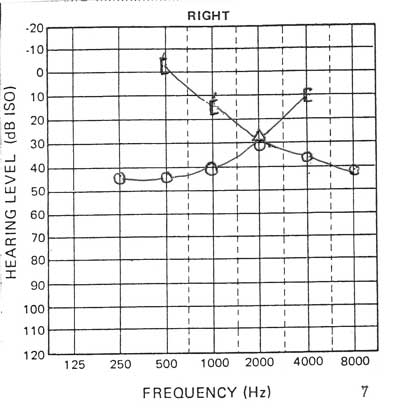
The loss of 40dB of Hearing is fairly significant too; this is indicative that the ‘cochlear tuning’ outer/inner hair cell function has been impaired.
If you have good insurance as with all forms of SN Asymmetry, you might want to get a scan done just to check that there’s nothing acting on your retro-cochlear function that’s going to get worse.
I’m assuming they mean “sensorineural asymmetry” - meaning the loss is sensorineural and not symmetric between your ears.
Yours is definitely not a typical hearing loss. It seems odd that is just came on suddenly - maybe it was caused by a viral infection of the cochlea? I’m not an ENT; just an audiologist.
I wouldn’t think otosclerosis - that tends to follow a different pattern, such as this - looks conductive except for 2kHz (this is the Carhart’s notch mentioned earlier):
Thanks for the reply. It might be from a viral infection - the chart you posted is definitely not how I’m hearing.The ENTs didn’t seem to think it was viral, though they haven’t been able to tell me what it would be, so I wouldn’t necessarily rule it out…
Not to harp on about this, but if my loss is sensorineural and down 40 db in the whole range of a male voice, why doesn’t my humming skew right like anything that enters my ears does?
When I google it it just tells me “deaf [as in sensorineurally deaf] people don’t hear their own humming”, which sounds promising, since my humming sounds exactly like it did before any of this started.
Maybe I have what Beethoven had. Good musical lineage there…
Your humming is not a Pure-tone signal. There will be elements of it above 750Hz, which you can hear bilaterally.
The intensity of the delivery of your own sound (partially delivered by bone conduction) is also much higher level than you think but your stapeadal reflex kicks in to reduce it.
I agree there. When, for example, I record my voice singing low notes, say 150hz, and play them back I indeed can’t hear the fundamental in my left ear but my brain reconstructs it from the overtones and the signal in my right ear. It’s an amazing testiment to the power of the brain.
That said, I’m a recording engineer with 20 years experience so I’m pretty used to spotting differences between L & R, I can definitely tell a difference when listening to that playback through headphones, for example.
In contrast, when I hear my voice through my head, with ears plugged, I hear zero difference whatsoever. Totally dead-centre mono from the lowest to the highest notes of my range. No dips, no bumps, and most importantly no distortion. It’s very possible in the lower midrange, like 150-250hz it’s actually a touch louder, like 1-2db, on the left. But if so it’s pretty subtle.
The discrepancy between the two experiences seems weird, no?
In terms of the stapeadal reflex, that term’s new to me, but interesting, and makes sense anecdotally from my training and exposure to loud sounds. Am I right in thinking it’s an overall adjustment of volume, not variable by frequency, and is the same in both ears?
There’s a bilateral reflex but it tends to dominate the ear perceiving the greater sound. You can feel it kicking in sometimes when you shout.
The difference in fully occluded listening is obviously not giving you the same roll-off as the Puretone testing.
This can happen with dead-spots in the basilar membrane. The top 40dB of your hearing is achieved via cochlear tuning. That mechanism can be flawed in the dead-spot, but that doesn’t mean you have no perception of sound. Contra-lateral cochlear tuning is also possible so when you start to hear a sound in your better ear, the inner hair cells serve to activate the tuning outer hair cells on both ears. However testing isn’t done in stereo, so the weakness of the IHC function is identified in your poorer ear.