We do all our testing with inserts anyway. Closed domes can be flawed due to pressure on insertion issues or leakage in tall narrow canals.
2 Likes
Does this imply that any PTA done without inserts potentially does have a risk of erroneous readings for lower frequencies?
There’s greater variation especially in the lower pitches when you use a headset. The assumed volume is around 5cc though that’s hugely variable, the clamping force will alter for different heads and some ears just don’t seal as well due to harder cartilage and voids in the skull shape.
Inserts aren’t perfect, but they do eliminate lots of sources of error.
2 Likes
Thankyou @Um_bongo and @Neville this discussion has helped me understand the inconsistency of AC at low frequencies better
I ran the In Situ yesterday and applied the changes. I like the results. I am a little concerned at how much worse my low frequencies tested.
I would hate to think my low frequency hearing deteriorated that much since last February. Can I take it from reading this thread that it is normal for low frequencies to be worse when using In Situ?

That’s meaningless without a BC figure - looking at it, either the loss has worsened or you’re testing under different venting conditions.
However, if you find the result more beneficial, you might be headed the right way WRT actual adjustment of the aids.
1 Like
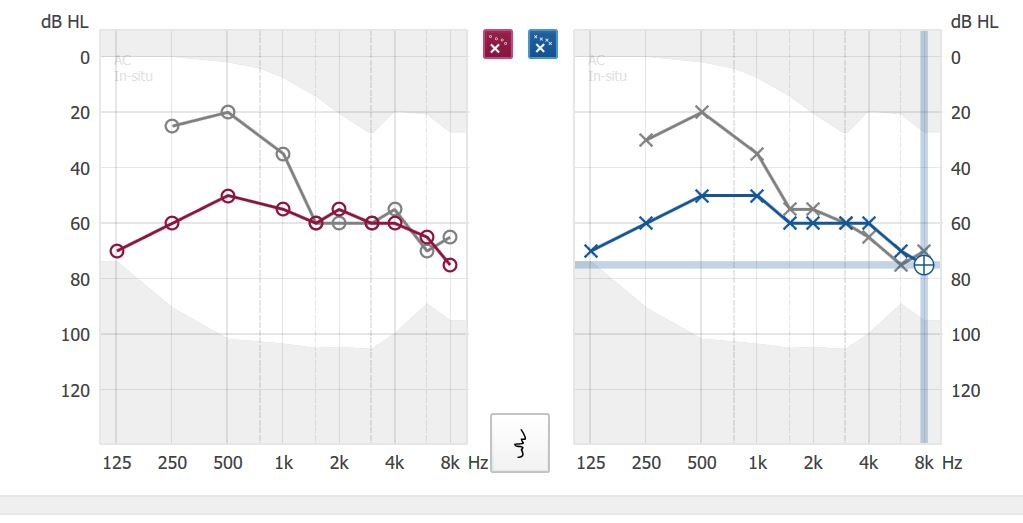
The original audiogram (grey) was done in a booth with headphones only. The In-Situ (red & blue) was done with with power domes in my family room.
I know the power domes leak because I have elongated ear openings caused by swimmers ear and they don’t cause occlusion. They do reduce feedback over bass domes though.
The audi did do BC testing for a couple of frequencies when she did the hearing test. She didn’t bother to document any readings because she said there was no problem.
I guess from what you’re saying, I will need to another hearing test done to find out for sure.
From Nov. 2009 to Feb. 2018 : I had a loss of 15 decible in the 250 & 500 frequencies. It would be worrisome to find I have another 15 decible loss in those same frequencies over a 9 month period.
I think it is the venting conditions that are responsible for the differences. I switched my 8 mm power domes with 6 mm double vent bass domes and ran the In-Situ Audiometry again. My results were even more varied in the low frequencies this time.
Note: I was wearing 6 mm double vent bass domes and still had power domes selected in Acoustics when I ran this In-Situ test.
I ran another test ( see my post below) where I have the same Base Domes selected in Acoustics and on the hearing aids prior to running In-Situ.
Choose exactly the same acoustic fitting in software before starting the insitu that you are actually using. Do the readings change when you change different types of domes and molds in the acoustics option of the software before running the test? If yes then the software is probably giving you improved results if you tell the software that you are using double vented but actually using a closed mold. Do share your findings
Ran the In-Situ again. This time with the Double Bass Dome selected. I did get slightly better results from having the correct domes selected prior to running In-Situ Audiometry.
I did the reverse. I was actually using Double Vented Base Domes, but still had Power Domes selected in Acoustics.
Note: The reading of 50 at 125 is wrong. The software wouldn’t let me increase to a db HL where I could hear the tone.

This might imply that software generates interpolated tones for lower frequencies . It might not be the real decibels but the equivalent decibels for the acoustic fitting selected. Do check again with double vent selected in software and the most occluding actual fit you can do (closed custom mold would be ideal but even power domes should do). I suspect it might take your results closer to the original audio gram .
I don’t think this is the case. I can decrease the db HL needed to hear the pulse tone by pressing on the Tragus and closing off any leakage from my ears. When I do this it takes my results close to my audiogram. This works regardless of which domes I have selected in Genie or have on my hearing aids,
This pretty much tells me my hearing hasn’t drastically changed in the low frequencies like I initially feared.
1 Like
Doctor it hurts when I do this. ![]()
Good news.
2 Likes
How does the first fit of the Marvel’s work in combination with an in situ?
My audi said that REM is old-school and that in-situ is the way things are done today. She has not done REM for a long time . Not sure what to make of that. I will be fitted for a new HA soon with her, presumably using in-situ testing. I am not sure if I insisted on REM whether she would do it.
The post by @Volusiano right at the beginning of this thread should answer that question.
REM is using independent, calibrated equipment to check that the output actually being generated matches the prescribed gain needed. It takes into account the specific acoustics of your own ear canals.
In-situ is perhaps faster and more convenient. Scientific and fail safe? Perhaps not.
3 Likes
It seems to me that an In-Situ test and a REM test is a totally different process measuring totally different things.
The REM test is a measurement of the actual sound level in your ear canal. They fit a microphone to pick up the sound level between your HA and the ear drum. Then a calibrated sound source at three different input sound levels (50, 65, 80 dB) is measured after your HA. These levels are compared to the prescription formula required for your hearing loss. Adjustments are made to bring the levels up and down to match the prescription curves. So, it is basically a test of your HA microphones, amplifier, and receiver, to see if it produces in your specific ear what it is supposed to produce. Because everyone’s ear is different, and there may be differences in the HA hardware, the output is highly unlikely to be what it is supposed to be. That is why adjustments are needed.
The In-Situ test on the other hand is really a test of your hearing assuming the HA produces a standard sound level. It probably does not because of the issues that the REM measures for.
It is possible that your fitter does not have the rather expensive equipment required to do the REM, or does not want to take the time to do the test and the adjustments.
1 Like
Yes they are different, but like you said above, ASSUMING THE HA PRODUCES A STANDARD SOUND LEVEL.
So in the REM case, if the HA does NOT produce the standard sound level, due to under amplification and/or canal size anomaly combination, then the audi does the REM direct adjustment to compensate for it.
In the in-situ case, any under amplification and/or canal size anomaly results in having to crank up the amplification to meet the threshold hearing level at the frequencies that underperform. Your new in-situ audiogram result in this case would most likely look worse then the original audiogram created by the audi in the sound booth. Then the re-prescribed amplification to the new in-situ result basically is kind of an indirect adjustment to the deficiencies in hearing aid under-amplification and/or canal size anomaly.
So while REM and in-situ audiometry are different things, they both can result in direct/indirect adjustment to address the deficiencies anyway, but in different ways.
And their 2 ways of adjustments may not necessarily result in a closely match final amplification result, because one is based on threshold detection (the in-situ audiometry), while the other one is based on normal levels of hearing (the REM), 2 different perception criteria.
2 Likes
Interesting thread.
I have never had the opportunity for REM adjustments. The two times I went to an audiologist for hearing aids REM was not done. I did get the audiogram results from these office visits.
Doing my own programming something I have learned is the in situ audiogram has proven better results with my hearing. I have used both the audiologist audiogram and my in situ audiogram for programming. This comparison of programming has been done on 6 different pairs of aids over the years with the same results each time. This discrepancy could be the needed REM adjustments we here so much about?
To me the in situ audiogram actually measures the hearing aid faults of domes, molds, tubing, receivers etc. to get an accurate threshold of the persons hearing loss with particular hearing aids.
I suppose this post is a little off base. Not a REM/in situ comparison.
1 Like
I found this University of Washington paper on how In Situ compares to REM. I posted the conclusion below. My summary of it is that the In Situ method MIGHT speed up the fitting, but it is not a replacement for REM and it is still necessary to do a subsequent REM if you want an accurate fitting to a prescription formula like NAL-NL2. The study was based on the Widex Sensogram In Situ method, and the REM was done to NAL-NL1.
Conclusions
The current study found that the expanded Sensogram™ does not create a fitting that is
closer to target than the basic Sensogram™, regardless of the level of technology. The analysis
did reveal that a measured Sensogram™ is more precise than first fit or simulated measures,
though the improvement was only seen at one to two frequencies. Moreover, the data also shows
that simulating a Sensogram™ by matching thresholds to the audiogram is less accurate than
using manufacturer’s first fit. Although measuring the Sensogram™ did result in mean REIG
data within 10 dB SPL of target data, the REIG was still significantly different from the NALNL1 target values. Therefore, the Sensogram™ cannot be used alone for fitting hearing aids.
Since the measured Sensogram™ only improves proximity to NAL-NL1 target values at a few
frequencies, it may represent a viable, but not crucial, shortcut for fine tuning with REMs. The
results from the current study reiterate the importance of using REMs with probe tube measures
for an accurate hearing aid fitting, even when utilizing in-situ measurements.