Im well behind that 75% number you mentioned there, so I should be a changed person if I get that much comprehension added back in.
I do a lot of home theatre tweaking as i have a decent setup, including Dolby Atmos overheads and multiple subs, so I use REW and room compensation curves, and I kinda understand the effect of frequency highs and lows on the sound outcome. I know, Im losing a lot in my hobby due to my hearing loss. I have hopes that I may get some of the benefit back - even some surround effects hopefully - if and when the aids get dialled in. It would be very satisfying for me if it did.
That, on top of better conversation following, would be the icing on the cake.
I like to remind new hearing aid users who are also experienced sound tweakers to not forget the wetworks. Your brain gets used to not hearing over a long time and when you put all of that sound back it can start out sounding tinny and sharp and weird. Resist the feeling that the hearing aid has to be tweaked for at least the first four weeks and just focus on consistent wear. Just like rehabbing a muscle that has been in a cast for years, the auditory system readjusts, and you need to give it time to readjust before you start taking away audibility.
@Neville do you think that prolonged wearing in my right ear will help, as you have mentioned above? Will any relearning happen there would you imagine?
I know theres a decent degree of loss there, but there are people on here with similiar (or worse?) who seem to get benefit from aid. Or is my loss more specific, being a single sided one.
Apologies if these seem to be very basic questions, but its confusing, baffling even for a newb to this like me.
It’s worth a try. My worry about that ear is more that is was sudden and that it was a while ago. Sudden losses are very commonly associated much more distortion and poorer clarity than more standard age- and noise-related decline, and clarity will also typically decline after a significant period of auditory deprivation. Further, because of the large asymmetry, you might also find yourself in a position where it is difficult to put in the work needed to adapt to sound on the right because it may interfere with your much better hearing on the left and make communication harder rather than easier. It would be interesting to know your masked maximum word recognition score on that side. If it’s currently, say, 60%, then there’s a much higher chance that with time and adaptation it might improve a bit and be beneficial, but if your WRS is currently 8% in that ear, then even if it were to improve to 30% that still so much poorer than your 90% left ear and it may remain unpleasant for you. BUT, it’s worth giving it a college try. I have patients with a history of sudden loss who do adapt well to amplification on that ear, and others who don’t, and others who don’t get a lot of communicative benefit but appreciate the balance and increased environmental awareness that it gives them. I have some who can tolerate nearly full prescriptive gain and others who cannot but still like a little bit of sound there, and still others who are able to tolerate more gain (and so more audibility) over time.
But given trial periods are what they are. . . is it possibly worth some $4000 to gamble on whether that ear will ever get to a point where you like using it? Knowing what I know about brain plasticity, my personal degree of tolerance, scientific curiosity and sheer stubborn perseverance, and living in my personal financial situation where that represents a considerable amount of money but not an amount that’s impossible to absorb, if I were in your position it would be worth it for me to put a hearing aid on that ear. But not everyone’s situation is the same. Additionally, you may not have to make that decision because it may be that you’ll know clearly one way or another within the trial period. Alternatively, you may find that adapting to the left ear, which you absolutely need, is enough work right now. Making a decision during the trial period to return the right one for now and keep the left until you are feeling comfortable with that one, and consider re-adding one on the right later, is also a perfectly acceptable decision.
As an interesting aside, cochlear implant candidacy for individuals with one poor ear and one good ear has been in flux. We are still gathering data on outcomes and I’m seeing change in candidacy in some areas and not others. Here on the forums you can see some people saying that they have been declined and others saying, “look at this one story of a guy who was deaf in one ear for 30 years and got hearing back with an implant”. But one of the concerns I think, or what has happened sometimes, is that when the implant is turned on you need to, to a certain degree, plug up the good ear and force the brain to figure out how to use the implant, which can take weeks to months. It’s one thing to do that when both ears are relatively poor and there’s not much of a choice, but when one ear is pretty good the brain can basically be like, “Hey, why would I do the hard work to figure out how to use that brand new signal when I’ve got this working ear right here that I already know how to use, path of least resistance and all that”, and so the brain never really figures out the implant signal. We don’t like to put the risks associated with surgery on someone when we don’t have a strong idea that the outcomes will be good, particularly when it’s elective and not life-saving. I’ve seen huge changes in candidacy criteria for people with bilateral loss over the past decade, and expect to continue to see changes for people with unilateral loss in the future.
Reinforcing what Neville said. My asymmetry is from an acoustic neuroma, and that left ear is basically trashed as far as recovering much intelligence with it. I’m using Phonak L90s and the one thing I can say is that all the phased array/spatial processing is a complete failure for me. So the even more esoteric features of something like the Sphere is likely of no value in my case. With your asymmetry, it’s hard to say but I have a feeling it would be a stretch to expect the beam forming and such to be of much benefit. But just having something audible in your weaker ear should be an improvement. (My next pair will be the low-end models…)
When one ear is unusable, it is often the case that speech in noise processing goes right out the window. The brain depends very heavily on binaural input for scene analysis. Loved ones can struggle to understand the impact of unilateral losses because the individual seems totally fine in quiet. Grief with a sudden loss often comes on a delay because the person thinks “well I’ve still got one ear” and only later comes to recognize the impact of losing binaural input. If you need a 20 dB boost in signal to noise ratio and a premium hearing aid can give you a 9 dB boost. . . it’s just not enough and you may be better off, as you say, using a lower end model in combination with a remote microphone system.
The sphere is a unilateral strategy and does offer a significant SNR boost. Though I think you’re right and in your case it’s still not going to be enough. It has been an interesting device for clinicians because some patients find it life-changing and others find it “eh”. One of the big factors does appear to be closing up the ear (more benefit from more occluded fits), which in the case your your right ear one really would not want to do. The OP’s left ear has more low frequency loss and might manage more of a closed fit.
The sound of my own voice is like Im listening to my voicemail message.
Overall sound seems a little ‘tinny’ - there seems to be not much bass or mid range, definitely less than i hear without the aids, even when I adjust the graphic equaliser. If I push the left dome in further to my ear canal, it seems to get bassier.
I have an open dome in left ear and a double one in my right.
The aids seem to lose connection occasionally, as in stop amplifying on my better left side.
Music seems to have less bass also, is there a way to improve this?
I have a 7.2.4 Dolby Atmos home theatre, I had hoped Id get the benefit of surround sound effects, but not seeing it as yet.
The audiologist said he would increase volume (or gain?) one increment each week for the next 4 weeks to give me time to adjust.
I’m having a follow up in 2 weeks time.
Its a mental shock for me to accept that I need hearing aids, more so then when I needed glasses. Not sure why that is?
Right now though, I think Im not seeing a lot of benefit for the inconvenience of wearing them? By that I mean, I think I hear ‘enough’ as I am, and the aids aren’t adding a lot?
Hard not to repeat what I said about my own experience in post #5 above: mostly be patient as your brain adapts to new inputs, and don’t fight (or be disappointed by) the earliest days of that process. Your brain will likely learn to ignore or downplay the parts of its new soundscape that it doesn’t need (the sound of your own voice, for instance). And your Audiologist has much greater control over improving your experience than the app alone offers when it comes to adjusting for music. But it’s a journey, not an instantly magic solution. Take notes of your experience and when you see him/her in a couple of weeks they’ll be able to make adjustments that will begin to move things in the direction you prefer.
On music specifically, and with the caveat that I’m not (yet) an expert: you’ve been living without a lot of mid-to-high frequency information for quite a while. The restoration of those frequencies through the aids is inherently going to make music sound different than what you’re used to. Some part of this experience comes down to “this (now) is more like what music really sounds like compared to what I’m used to, but I miss aspects of the sound I heard before the aids”. The open dome in your left ear is letting in the lower frequencies that you’re naturally able to hear while amplifying the higher ones, so external music is going to sound brighter initially and potentially overwhelm the lows/bass. Pushing the left dome in further is really (I think) essentially closing that dome to the outside world, giving you an experience more like earbuds or headphones which often sound better for music.
It’s hard to put into words, but again there are two things going on: your brain is adapting + the aids are compensating for the state of your hearing loss at inception. As your brain adapts, the appropriateness of the initial settings will drift apart from optimal. That’s paradoxically both a) why you should wear them as much as you can to help your brain adapt faster and b) why your audiologist will make adjustments to improve your experience as that brain adaptation continues.
Also: If you’re streaming music to your hearing aids, adjusting the Ambience slider in the app can greatly improve your music listening experience by lowering the volume of the mics/outside world the aids are mixing in with the streamed source. And… you can often adjust the e.q. more broadly than the myPhonak app at the streamed music source. That’s probably also true with your home theatre setup: if it won’t annoy others, try making e.q. adjustments there rather than in the hearing aid app.
Not really. I am asymmetrical and Sphere is the only HA that can use unilateral AI.
Oticon Intents, Starkey Edge AI and Resound Vivia seem to require binaural fitting to achieve the full potential of their DNNs. For me Phonak Sphere it’s probably the only option.
Lol, story of my life during 2013-16, when I was trying to learn to hear with a CI, but without isolating my better ear (I was one of the first CI recipients in my country with a relatively good other ear).
So, probably you’ve said in the past and I’ve just forgotten–what eventually got you to isolate the CI ear and how long did it take for it to start working for you? I’m sure I remember correctly that you do well with it now.
I stream practically to the CI only because of my willingness to rehabilitate more effectively. If I cannot understand, I switch to phone speaker or hearing aid side only (Phonak Paradise 90-RT).
Theoretically, with a Cochlear Phone Clip (an intermediary Bluetooth Classic device), I can stream binaurally, but I found it cumbersome. I haven’t yet found a way to get binaural streaming with Bluetooth ASHA to CI and Bluetooth Classic to HA.
The Phone Wireless Clip battery lasts 5 hours now (8h after receiving), after heavy use (IIRC, Ni-MH), so recharging it is also inconvenient. The Nucleus 8 sound processor is definitely more convenient with direct streaming, which translates to more hours of rehabilitation.
I bought a Cochlear Wireless Phone Clip (described above) and it stubbornly and consistently streams only to my Nucleus 6, for example, when I return from work. Streamed a lot whenever possible, because it’s basically the only way to isolate my better ear.
I requested a custom silicone earmold, which functions as an earplug specifically for my better ear, but it only offers approximately maximum 40 dB of attenuation, so it is not perfect for isolation.
Hard to say, because although I didn’t regain usable hearing during 2013-2016, it provided some foundation for further training after the subsequent 6.5-year break.
I gave it a try because @Raudrive, in private messages, discerned between the lines that I was dissatisfied with my results, and he recommended that I isolate my better ear… IIRC, this was in March 2023.
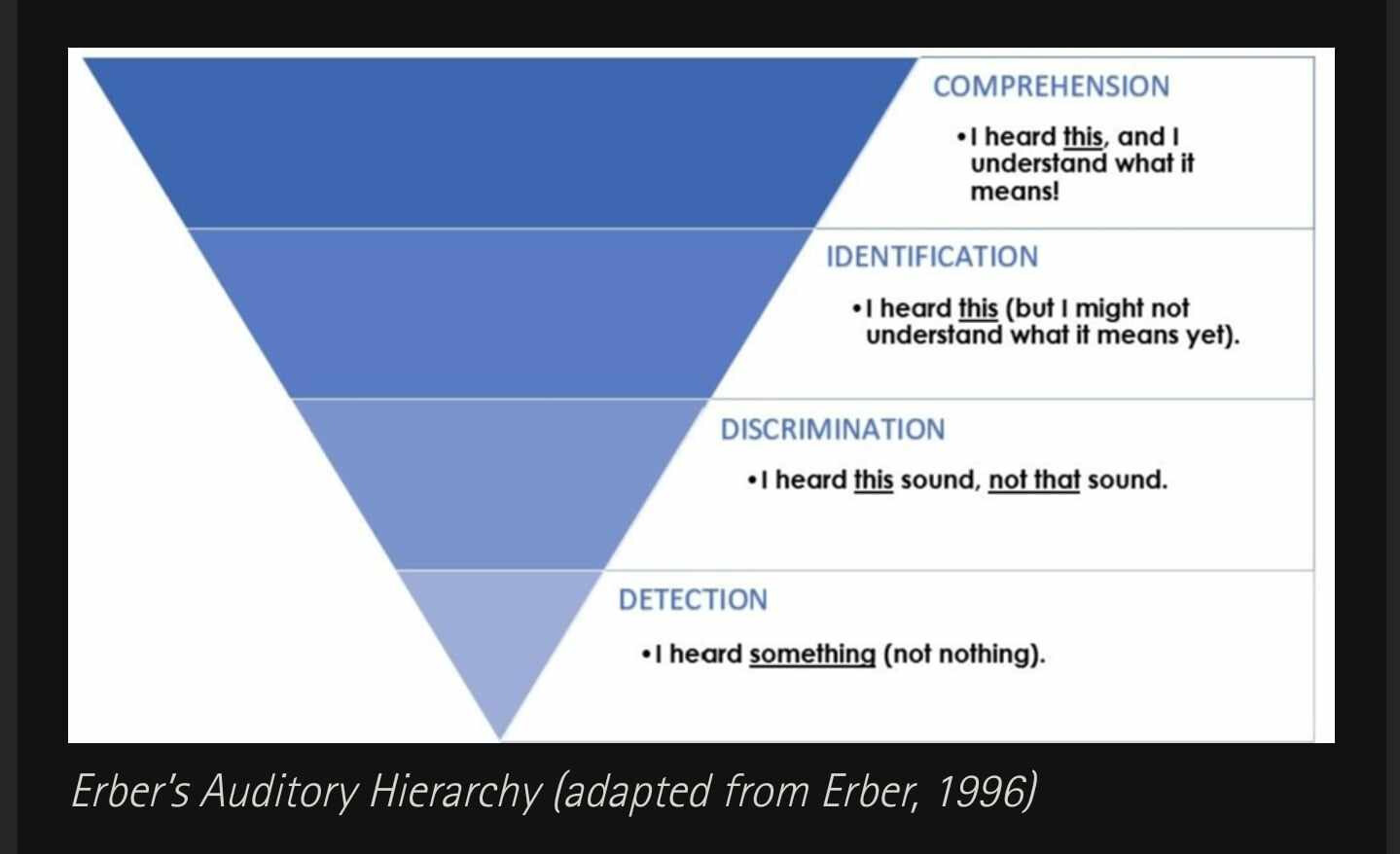
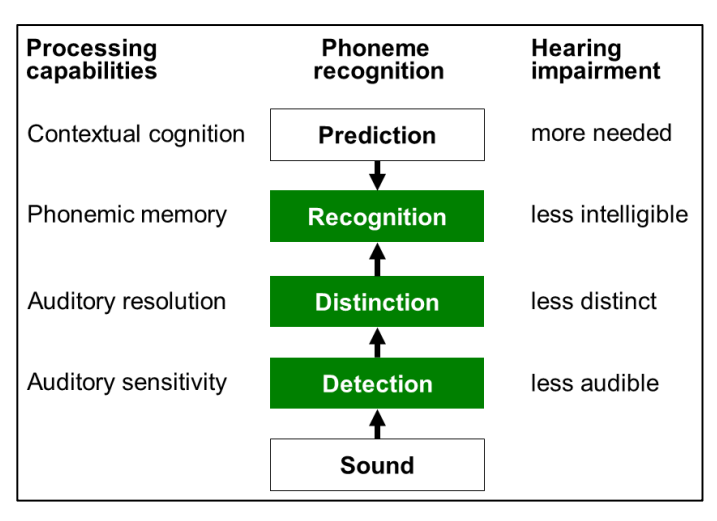
After consistent heavy streaming - I need a few months to achieve reception of sentences, but not perception yet. See screen below - I mean “Identification” and “Distiction”.
Now I am gradually transitioning to “comprehension” and “recognition”.
.
See my post; it describes WRS in January 2024, ten months after @raudrive’s advice. During that time, I had a three-month gap due to studying for an important exam—keeping CI working was exhaustive…
In fact, I’ve only been able to track someone’s speech in a quiet environment for about a month now using only the processor’s microphones. I wasn’t able to do that in early December.
Rehabilitation is easier and more convenient with the Nucleus 8 sound processor, which I have had since October 19, 2024.