I’ve just got myself an ear mold from the NHS with a 1.5mm vent. I’ve never had vents before in my life. My hearing in my right ear has improved since surgery.
When the NHS adjusted my NHS hearing aids to accompany a vent, it has a flat line at 0 dB up until 1000 htz. Is that because I hear below 1000 htz naturally now through the vent?
Also hearing through my Roger System now sounds a bit weird, is that because of the flat line up until 1000 htz?
When I mute my aids, I can hear some what but it’s very little.
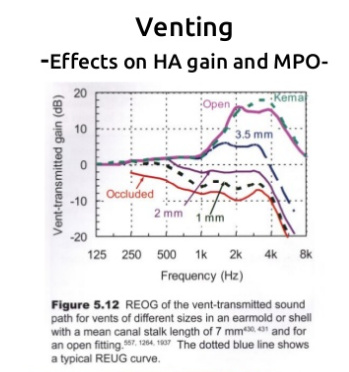
I presume you are talking about your right ear only, and the left ear has no vent or a very small vent? On your right ear, a 1.5 mm vent is still a small vent. You will get some natural sound through it, but not a lot. If it were larger it would let in more high frequency sound, but not much different at low frequencies. I have saved this useful slide presentation on the impact of venting on hearing aid performance.
Click on that link I provided and look at the whole presentation. Venting is complicated. I believe in some case where space is a problem they can make the mold with a “trench” down the side of the mold where it fits in the canal to make the vent bigger. May not be something that NHS does though…
I’m just winging it, but I think a larger vent allows the natural acoustics of the ear canal to function. The natural acoustics give about about a 10 dB boost at about 3000 hz. This shows up on a REUG (Real Ear Unaided Gain) test.
The bigger effect is receiver loss of gain as the vent increases. It is hard for a small receiver to develop significant sound pressure at low frequencies when essentially all the sound is “leaking” out the vent. As the frequency increases, there is a resonance point, like in a vented port stereo speaker, but due to the small ear canal volume, at a higher frequency. So you have a combination of the receiver becoming more effective as the frequency goes up (less leakage) and the resonance effect. The fitting computer program attempts to correct for all of this stuff based on theory. However, what you get is going to depend on the actual ear canal size and where the fitting fits in the canal, etc, and what comes out of the is the sum of all these effects. That is why we need REM. It measures what you actually get, instead of what the theory predicts. Then of course the fitter can then adjust gain to get what we really want for sound level vs frequency.
Or, at least that is the way I have rationalized it.
1.5mm is very small, almost occluded. My silicone molds have either 1 or 1.5 mm vents and I hear almost nothing when the aids are muted. As an experiment you might get into the software and temporarily change the vent size and see what the gains do.
Your weird sound from the Roger I would think is due to the lack of gain in the lower frequencies that you are accustomed to.These new NHS aids, are they the same as before?
There are three major types of vents found in a hearing aid shell or earmold: parallel, diagonal, and trench. All three vents are designed to accomplish the same thing, which is to provide some reduction of amplified low frequency sound—that is, allow low frequency sounds to leak out of the ear. Venting also allows for some pressure relief, which results from bone-conducted sound getting trapped in the closed-off ear canal when a tight-fitting hearing aid is inserted into the ear canal (the sound is generated from the condyle area of the mandible, which is located close to the ear canal). This problem is especially apparent when patients talk or chew.
The most commonly used vent is the parallel type; however, there are instances when a professional may have to substitute a different style vent. It is easy to forget that the vent type can have a significant effect on the reduction in low frequency energy, as diagonal vents reduce low frequency energy more than parallel vents with the same internal diameter. This is illustrated in Figure 2, which compares the same hearing aid with identical acoustical settings. The only change is the style of vent.