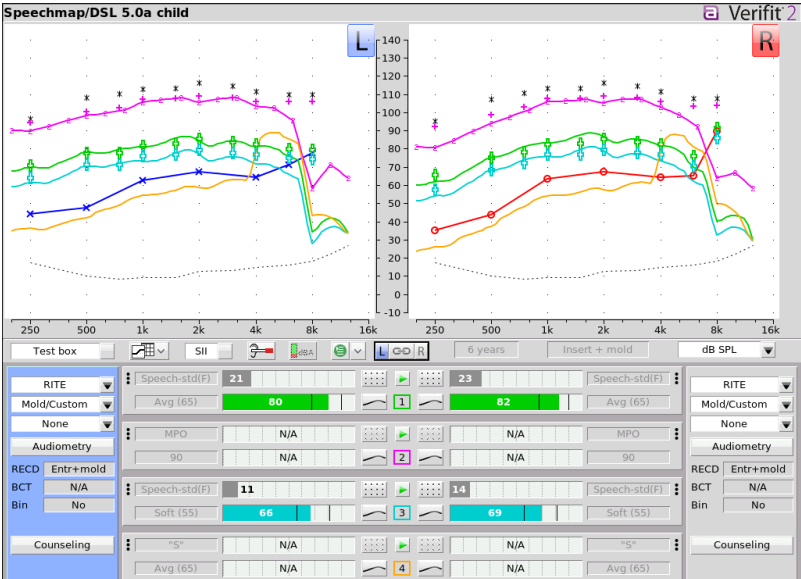
Others are correct that historically it was difficult for hearing aids to amplify up there, there are diminishing returns for speech up there and increasing patient complaints and feedback issues. But. . . just to be devil’s advocate, frequencies up past 4 kHz are what resolve phoneme confusion for sounds like /z/ and /p/. Pediatric targets chase them and, regularly these days, get them. Note that these are DSL child targets rather than NAL-NL2 targets.
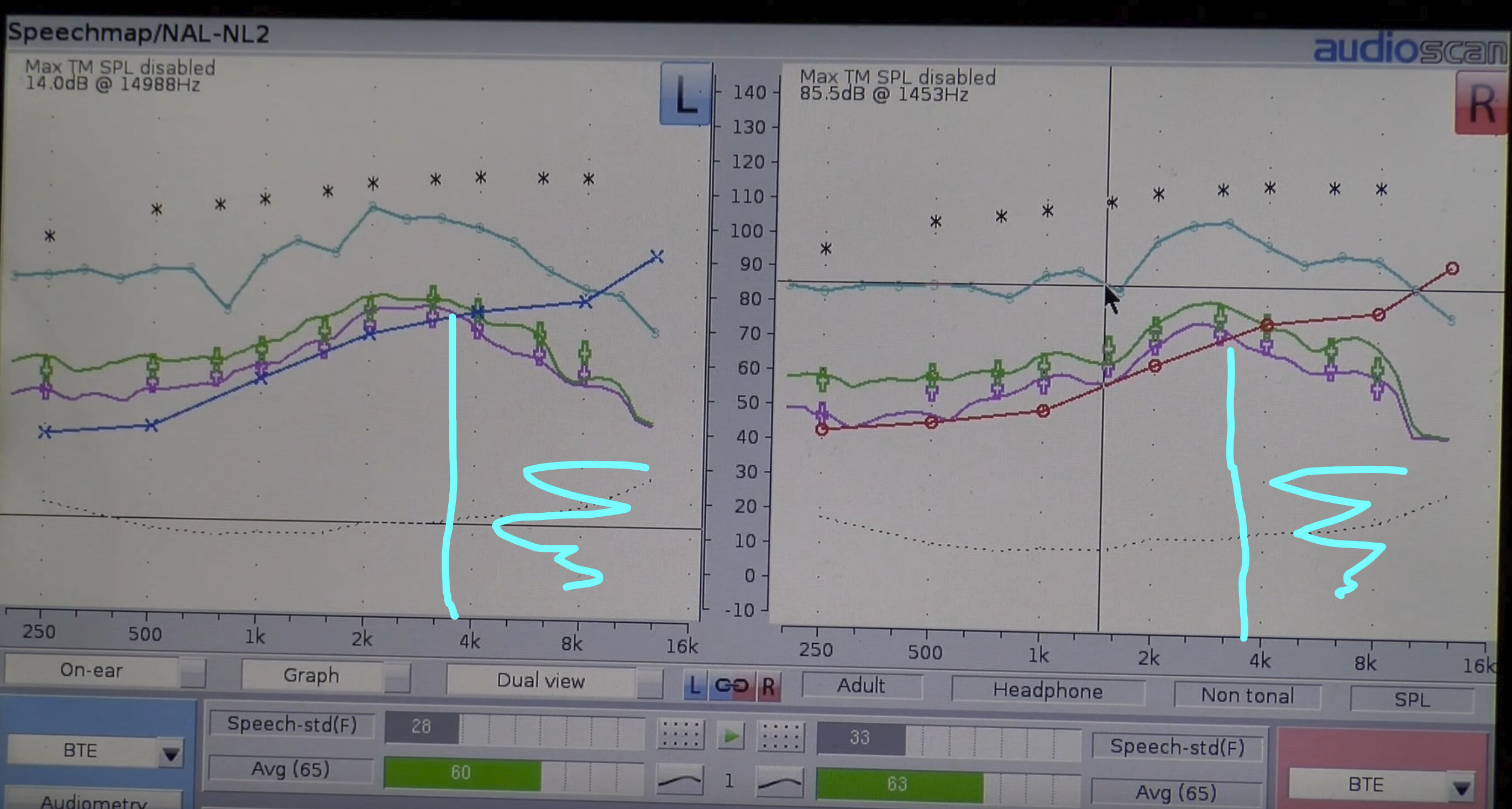
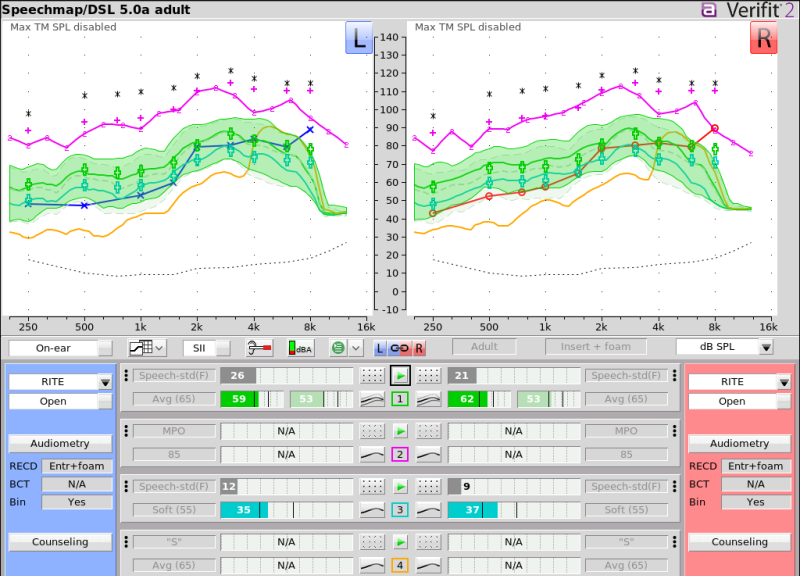
You can also compare DSL 5.0 Adult targets, which are closer to NAL-NL2 but still provide a bit more high frequency audibility (compare to Baltazard’s original snap). These are rechargeable RICs, a few years old (not current), custom tips M receivers. In this case, there’s some feedback limiting around 6/8 kHz with the current acoustic coupling.
Compare, also, the speech intelligibility index for the pediatric targets is about 80% whereas for the adult fit it is about 60%.
And for added interest, for those of you familiar with software targets, here’s a snap of the settings that were required to meet prescriptive targets for one of the above–significantly above what the software thinks it needs.
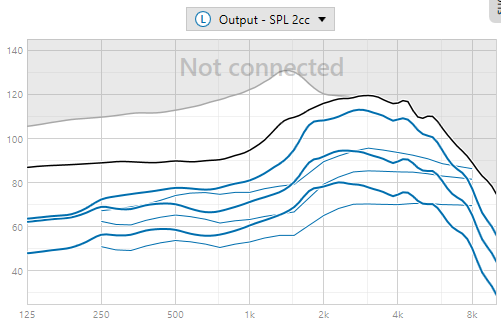
You’re not going to get that without REM. No clinician would push the highs that dramatically without being able to see what was happening in the ear. Additionally, clinicians who don’t do REM actually have no idea how far below targets hearing aid gain can (regularly) be.