Philips 9040 fitting at Costco by a very conscientious HIS almost at the end of an apprenticeship period. Below are before and after REM insertion gains. Philips 9040s with microShell molds, all settings at defaults; Fit4Speech rationale, Frequency Lowering. Are the high-frequency additions by REM, up to +28 dB, plausible or did I screw something up in preparing the spreadsheet for the calculations?
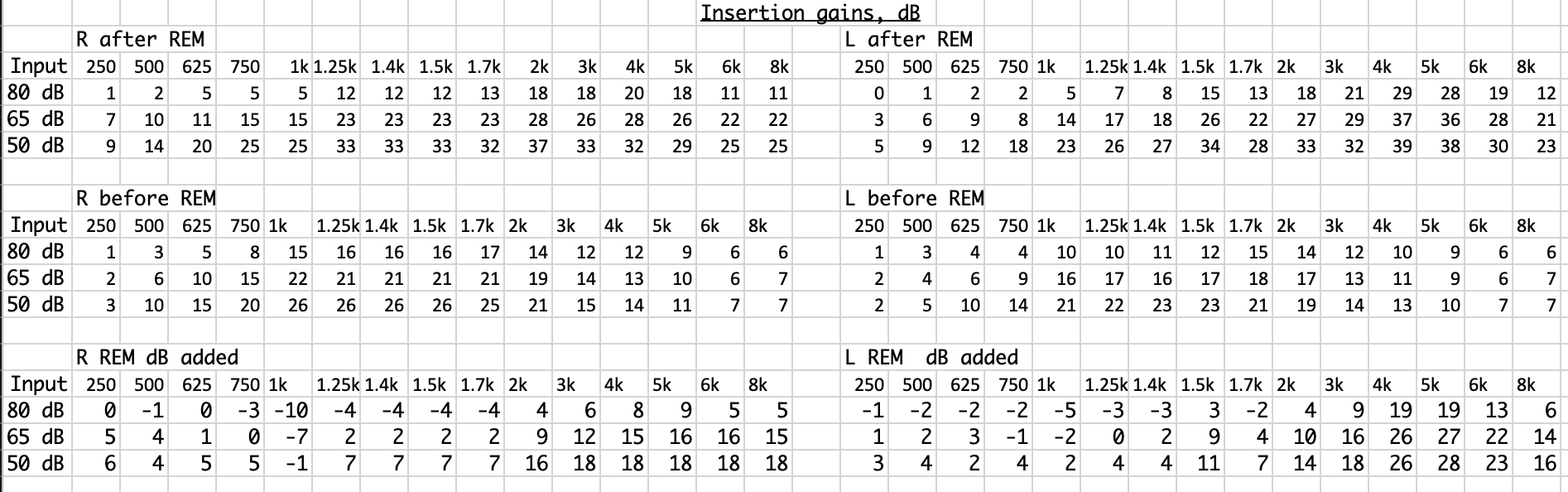
Both ears are consistent as far as needing gain for REM.
That should be very noticable to you. Did you get a chance to hear before and after REM?
The signs pattern is roughly similar between ears, but my question is about the magnitudes – whether +18 to +28 is plausible. Of course the REM boosts are noticeable.
Looking at the before REM it looks like they’re programmed for somebody new to hearing aids and likely with the settings for open domes. (There’s not near enough gain to make the high frequencies audible) After REM numbers look reasonable for molds and full gain to make those high frequencies audible. TLDR: Yes, I think REM really did aid that much gain. The “First Fit” had you way underfit.
Fit4Speech predicted targets are different than NAL-NL2 so when performing REM, it would have likely been adjusted to match the NAL measured targets. I’m definitely an advocate for NAL-NL2 targets so I would say it looks like they did a good job. I’d be interested if the REM was performed with the frequency lowering on or off, and possibly suggest asking for an additional program with frequency lowering off but all the other settings the same.
Note that the numbers in the software don’t always indicate dB. They may just be “steps”.
2 Likes
Before REM had acoustics set to actual (molds), experience long-term, no acclimatization, with Philips’s Fit4Speech proprietary rationale.
Regardless, “REM really did [add] that much gain” is an answer to my question.
I think the HIS may have mentioned that the REM fit to NAL-NL2. I think I’ve also seen somewhere that some REM equipment is limited to NAL-NL2 and perhaps other standard – non-proprietary – rationales. That raises the question: what’s the point of the fitting software being set to a rationale different from what REM is going to use as a target?
1 Like
It is a good question, and not one always answered well by the manufacturers even. I’ve seen studies that suggest that hearing aids properly fit to NAL-NL2 outperform ‘major manufacturers’ hearing aids fit to proprietary formulas. The studies almost always obscure what brands and models that they tested, unfortunately. And then the brands have their own studies that usually include a group of like 8 people who did better with their proprietary formula and it never seemed clear to me whether the fitting was verified by any probe mic measurements. I know that isn’t really what you asked, but you should know that this question is also asked by people working in the field. Even though it is a simple question, I think you would be surprised at the variety of answers you would get.
Functional gain provided by the hearing aid can vary widely from person to person due to their anatomy. If it isn’t measured, it could be off by as much as 10dB or more from what is expected. So any formula that is used should be verified. The most common suggestion for ‘best practices’ is probe mic measurements.
Depending on the audiometer used and the fitting software, you can either establish manual targets or some fitting software will include a way that the software can connect to the equipment and it will tell the equipment what targets it is trying to match, basically. In Philips software, there is a tab under the Fit Instruments section that says REM. In that screen, you can select Real Ear Fit. This could allow for a probe mic measured (REM) to be performed with the selected fitting rationale, such as Fit4Speech.
I would like to reiterate that I think NAL-NL2 does a great job in a significant amount of cases, and when it is used by a skilled HIS. If you are hearing well with the hearing aids, I think there is a fair reason to suggest that you should keep those settings. I just wanted to share information since I also think it is good for people to be informed, especially those that are taking their time to seek out that information.
Please be kind to your HIS even if they are not aware of some of this information. I know for a fact there are some members of this forum who have much more knowledge than I do so if they would like to correct anything I’ve said, that is ok too.
1 Like
Noted, 'though for Philips HearSuite one step of adjustment – one click on an up or down arrow – is one dB.
(NB I don’t know what I’m talking about; this is layperson reasoning…) It could allow that, but only if the REM equipment has the feature of accepting targets from the fitting software. Some does, but whether Costco’s does I don’t know. I did notice that the HIS manually adjusted the gains in HearSuite after the REM magic, although this doesn’t necessarily mean that targets were not transmitted.
A little off subject, but are these REM corrections applicable if you use Sound Recover or frequency shiftting? Is NAL-NL2 as significant when using frequency shiftting?
1 Like
Frequency lowering with Probe Mic Tubes
Purdue frequency lowering assistants
These would be my suggested materials to read more about frequency lowering. Yes, REM is still an important part prior to utilizing frequency shifting.
1 Like
I am going to show my ignorance on this probably.
Why would you set up REM prior to the initial
programming of the hearing aids?
The rational of using frequency lowering is for those with little to no hearing in the upper frequencies. Purchasing SP or UP aids to cover those high frequency losses is foolish. Why set up REM before setting up frequency lowering programming?
Thanks
In the procedure recommended at the first link provided by @mindsil, an article by a professor who seems to specialize in freq. lowering, freq. lowering is turned off before REM is done. Then it is turned on and the probe mics are used to adjust and assess the freq. lowering parameters.
That many practitioners follow a procedure like that seems doubtful to me.
1 Like
In this case, REM does not mean that you are focused on making every frequency audible. Often NAL-NL2 will drop the high frequencies. There is some information out there concerning the fact that a hearing loss above a certain level in the high frequencies may lead to sounds being distorted once they are audible and it can make speech comprehension more difficult.
The REM is important so that you have verified the output of the hearing aid and what is actually making it near/to the eardrum. That way you can calculate the maximum audible output frequency to determine the minimum amount of frequency lowering necessary. As the article talks about, it also depends on what technology that brand uses for their frequency shifting/lowering/compression.
In general, if you aren’t going to verify with PMM what the frequency lowering is doing, then it is probably better to leave it off. This is a generalization but a pretty good one.
I would agree that very few clinicians use REM to set up frequency lowering. I think most typical is to turn it "on, " hear you don’t like it and turn it back off. I think using REM is the ideal way to set up frequency lowering, but trial and erroring until “s” sounds sound like “sh” and backing off a bit until they sound like esses again does a decent job. This is assuming profound high frequency loss. I guess first one needs to determine if one might benefit. Another approach would be to start with very mild settings and gradually increase.
This doesn’t make since to me. Why do REM twice? The first one without frequency lowering is a waste of time. Or am I missing something?
This got a chuckle out of me. You need to understand my hearing a little.
I can see setting REM while using frequency lowering or just not using REM on the upper frequencies that the patient can not hear well. that makes since.
The idea of doing REM initially without frequency lowering is to get an idea of how high of frequency the aids can make usable. Then repeat REM after frequency lowering is set up to make sure you didn’t make things worse. I’m convinced very few, if any do this unless they’re the people researching it like Josh Alexander.
1 Like
My thoughts were that’s what the audiogram was for but your point makes since.
Thanks
2 Likes