I’ve been a longtime reader of this site and have noticed multiple requests either searching for analog hearing aids or asking for ways to make digital devices sound more analog (similar threads can be found on Reddit and other forums). I have also spoken to dozens of audiologists across North America, all of whom get repeated demands for analog hearing aids.
It is clear, in other words, that there is an actual market for these devices. As a lifelong wearer of hearing aids who grew up on analog, I know well why these requests keep coming up. What I am trying to figure out is how we might productively signal to the manufacturers that such a market exists.
I am not trying to start an analog vs digital debate – I’m not saying digital devices shouldn’t exist, just that analog devices should as well. I am happy to discuss the reasons why many of us prefer analog sound if needed.
Suffice to say, I don’t believe there is any good medical or audiological justification for completely phasing out analog hearing aids. So I would like to use this thread to discuss ways that we might demonstrate to manufacturers that, if just one of the major manufacturers made just one analog line, we would buy it!
I have tried circulating a petition here, but it seems that the forum bots don’t like links. Any advice would be much appreciated.
I’m 100% on board with you on this. I have (what I consider) severe tinnitus 24/7 along with RSHL and analog aids (Phonak Lyrics) calm the tinnitus and allow me to hear very well. I have trialed 6 or 7 digital aids and none truly work for me.
I think you have a tough hill to climb. I also suspect it comes down to cost and performance. Probably manufacturers would not admit it, but I wouldn’t be surprised if analog hearing aids, especially if you have to start over with the design, were not more expensive to make. And, then while there are some who are adamant that they want analog, it probably does not add up to a very significant demand.
If I could make a comparison to vinyl records and digital CD (which are now essentially obsolete too…), it would cost me about $1600 to replace my existing analogy vinyl playback system from the 1980’s. A very well designed musical CD player is $400, and a component CD drive for a desktop computer is probably $15. While there are vinyl purists, and the market still exists, I would not bank on a comeback of vinyl.
And I think your last problem are the electronics design engineers who design these things. I am sure that they will swear on a stack of bibles that they can made a digital HA that is not only equal, but far better than an analog one. There would just be no interest from them.
It’s pretty simple: you either tell the aid to act in a more linear fashion in the prerequisites or just let it default a gain setting, then go into the advanced gain adjustments and set the higher gain values the same as the G50 while winding up the MPOs to their maximum and turning the feedback manager off.
If you do this in a nominal music program, you’ll also inhibit a significant amount of the noise management and speech enhancement too.
You’ll have a nice linear sound and very loud sounds will be very loud. This will probably give you more feedback, auditory fatigue and may result in more long term damage to your hearing.
The only people who should be asking for a fully linear aid are those with a purely conductive loss. For everyone else it’s an impossible goal, due to recruitment. However there is merit in asking for an aid to be more linear in order to preserve normal loudness growth - apply judiciously
I’m sure you’re right that this will be a long process – I don’t expect it to happen overnight. But I would note that in fact vinyl has already made a comeback – vinyl sales have gone up about 1000% over the past 15 years. It still represents a minority share of the market, but its sufficient to make the recording industry press vinyl again. I see no reason why this couldn’t happen with hearing aids.
I also suspect you’re right about the engineers, but they’re mistaken, and they’re making the same mistake that the audio industry made many decades ago. If you ask most sound engineers and masterers today, they will tell you that analog is the gold standard.
Many thanks for this response, but I want to point this out because its important: linear programming will help with some of the more bothersome aspects of digital sound. But it cannot fix the biggest problem, which is the removal of sonic information by the digital sampling process. It is the loss of that sound (and the extra work the brain has to do to compensate) that causes the biggest problems for hearing aid users who prefer analog.
I used to be a hard core audiophile, but with my hearing loss that interest is fading. I’m a bit out of touch with the recording industry, but I suspect 99.99% of masters are made with digital recording. Even back when vinyl was in its heyday, the best masters were made with digital recording, and then the vinyl was pressed from that. There were a few masters made with the direct to disk process where no recording was involved other the the master disk. However, that is very difficult and expensive to do.
I am afraid that I am in the camp of those that say there is no loss in the sonic information with A/D conversion and then conversion back if it is done right. Digital is a lossless process.
Well, I am a hardcore audiophile and I have profound hearing loss. For what it’s worth, more and more masters (as well as reissues) are using analog tapes, and AAA vinyl is generally considered the best. I admit I don’t agree that the digital conversion can ever be lossless. That said, it is certainly true that one can sample at less “lossy” rates. As it happens, however, digital signal processors in hearing aids are incredibly lossy. I do hope this changes.
And of course, if you’re happy with your digital aids, great! It’s just that a lot of us aren’t, and it would be good if we had a place to spend our money.
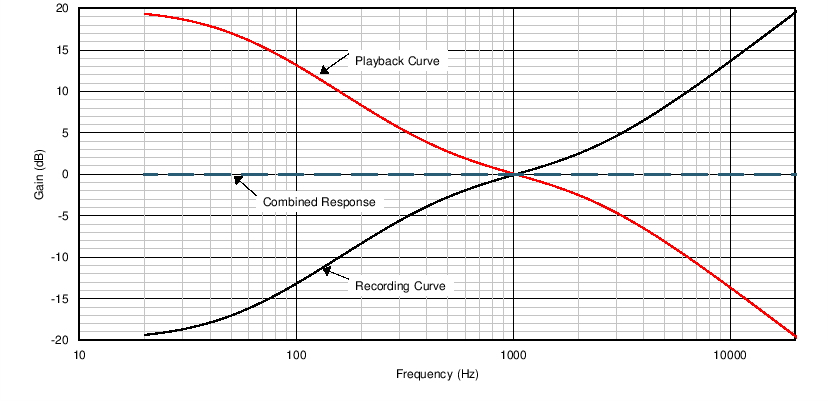
Some consider the vinyl recording process to be “pure”, but I would suggest it is far from pure. If the vinyl gooves were recorded full scale you would not get anywhere near the amount of music on one LP. For that reason, low frequency sounds are compressed for recording and then expanded again during playback. See the RIAA equalization curves.
And if tape is used then some kind of noise reduction like Dolby will need to be used to reduce the tape hiss and provide reasonable dynamic range. So again in the tape phase low amplitude sounds are amplified during recording and then reduced on tape playback. This can lead to the pumping that we can also experience in hearing aids when noise reduction is used.
My point is that with wide dynamic range digital, none of this compression and expansion is needed based on frequency (vinyl stage) or based on amplitude (tape stage). The pure analog signal is converted to digital without any compression and decompression. That said, many CD’s and especially the pop stuff intended for use in cars are highly compressed. If it wasn’t you would not hear any of the quieter stuff due to background noise.
But, we digress. I remain unconvinced that digital destroys any sonic content. There are some issues like Jitter that can be a problem if the hardware is not designed to eliminate it, but for the most part digital processing is pretty well done.
Well, I could probably argue about this all day, but this is getting pretty far afield. More to the point, most of these claims about digital tech are moot when it comes to hearing aids, for the simple reason that digital aids do not actually offer anything like the sound quality of other digital recording devices. For example, the DSPs in hearing aids have a sample rate of about half that of a CD.
There simply is no wide dynamic range digital when it comes to hearing aids at this time. Again, if you’re happy with your hearing aids, that’s great. But many of us aren’t, despite many attempted fixes, and I would like to see that changed.
My understanding is that the lowest bit level used in hearing aids is 16 bit, like the CD quality standard. And some hearing aids have been using 24 bit sampling for some time now.
That number refers to the bit depth, not the rate. Digital aids sample at a rate of about 20 kHz per second, whereas CDs sample at 44.1 kHz per second.
I’m very curious about the analog-vs-digital preference.
Seems to me you could tune a digital HA to give the same response as the analog with the proper digital filters. Digital filtering has become very sophisticated. (This is my current business.)
Perhaps the digital filters are not sophisticated enough to reproduce the phase relationships in the sound waves that the analog filters do, or perhaps the EQ curve just wasn’t set in the same way.
It would be interesting to do some calibrations and A/B test a digital and analog HA with the same domes, same receivers, etc.
My understanding is that the more recent and advanced systems of analog to digital conversion uses sigma-delta 1 bit at much higher frequencies. I do not claim to understand it all, but I think the older multi bit methods measured the full voltage at each sample point, and the more bits you used the more accurate the conversion. With sigma-delta you measure the voltage much more often and only measure the difference between the last sample point and the current sample point, and because you are measuring a much smaller amount only 1 bit is required. Hearing aid manufacturers are not very forthcoming with this kind of detail about their aids, but I believe some are using the newer sigma-delta method.
If it’s designed properly with good Nyquist anti-aliasing filters ahead of it, the delta-sigma ADC should create a very faithful reproduction. We use them all the time with phase and distortion sensitive biomedical signal digitizing and they work great.
If I had to put money on it, I would bet on phase shifts in the digital filtering causing a difference in the “feel” of the sound. You have to use more computationally expensive FIR digital filters with longer latencies to preserve phase information rather than the simpler IIR filters that have shorter latencies. So it may have been a tradeoff for computational cost and short latency versus phase fidelity.
Many thanks for this – it’s very helpful to get input from people involved in engineering. This difference may be one of purpose --i.e., biomedical signal digitizing may require different outputs than human hearing, day in and day out.
It also may indeed be the case that improvements in digital filters would go a long way here. But speaking as someone with a strong preference for analog, the difference is not small as things stand right now. Even when programmers adjust for compression and the like, there is still a noticeable absence of detail and clarity in digital sound, and I have noticed this across multiple hearing aids, all at high costs.
I assume this has much to do with the sampling done by the digital signal processor: by the time the signal is reconverted to analog and sent to my ears, the acoustic wave is a much-reduced thing. This is most noticeable when listening to music – e.g., John Coltrane just sounds thinner and less lifelike. But even in the course of an ordinary day, I notice fatigue by the the end of the day: my brain just gets tired of constantly filling in the sound that’s not there.
I too, feel hearing/ear fatigue by the end of the day with my digital aids. I literally have to pull them off every night around 9pm when my wife and I often like to sit and watch TV. This leads to us having to crank the volume to uncomfortable levels or to me throwing on my wireless (Analog!) Sennheiser headphones which I love but my wife hates since it reduces/removes regular conversation between the two of us.
Do you suffer from tinnitus and/or RSHL like myself? Just curious.
Thanks.
Mark
I would suggest this is a problem you are creating for yourself. Modern high fidelity analog to digital and digital to analog conversion is done without any loss. When high fidelity audio is compressed to iTunes, MP3, Spotify, and other compressed formats there is a loss of data and fidelity. Most do not hear it however, even in this extreme.
Audio is simply a fluctuation voltage signal. All digital does is sample this voltage up to 192 thousand times per second. With a 12 kHz audio signal which is about the upper limit of hearing aids that is a sample frequency of 16 times per full cycle of audio. With filtering that is easily enough information to recreate the full cycle of voltage. Part of the filtering and smoothing can be the receiver speaker itself. It cannot follow higher frequencies and as a result dampens out any higher fluctuations in the signal. It is a mechanical/analog filter in effect.
As Haggis has mentioned there is the issue of phase coherency. That is much more complicated and controversial. That is where there can be some differences in how an analog signal is processed. Equalizers were the big enemy of phase coherency, and many, me included refused to use equalizers. However, if you look at a recording studio panel, it is one huge equalizer. Phase coherency may have been destroyed long before you get the audio to your ears. A hearing aid is a programmed equalizer, and regardless of whether it is analog or digital phase coherency is probably the casualty of the process.
I have read about some of the old time hearing members who came up with analog aids becoming hearing aid self programmers. Because of their unhappiness with digital aids they decided to start self programming.
This might be a way for you to figure it out. Other members like yourself have done this with good results. The information needed to do this is in this forum. You just need to research and learn. Others have done it.