Still learning, one week in on my Jabra Pro 20’s. I have a question I need someone to explain to me like I’m five.
How do hearing aids work? This is simplified, so let me explain why I ask this. Remember when we were not as in tune to our hearing, and listened to loaud music in the car. Next morning, upon cranking said car, the stereo was alarmingly loud. I’m getting a similar sensation with my new hearing aids. I was told this is normal, and I’d grow used to it.
Here’s what I know. My audiologist set me up for 4 weeks in acceptance manager at 90% of prescription. I’m one week in, so if linear, that should put be about 92.5% of gain. My target rule is NAL-NL2. I have no clue what that means.
So, here is where I’m breaking down on understanding. As you can see from my posted audiogram, I have loss of about 50db from about 1500 to 4000 hz. That means I can’t hear anything below 50db I’m assuming. So it’s amplified. Just for simplicity, let’s say 2000hz is 50db loss and I hear a 2000hz sound at 60db. Does the hearing aid amplify that 2000hz sound above 50db by reproducing a sound at 110db or whatever the uncomfortable threshold is set at? How is all that calculated, and is my hearing aid going to make me have more hearing loss?
Okay i am going to start by saying you have what is known as a cookie bite hearing loss. By the way that is how my hearing loss started too. I believe that your audiologist should have started you out at 80% of your prescription, at least that is where I was started at. And still everything was way too loud. If it is too uncomfortable for you I suggest to lower the volume of your aids say to -1 or maybe even -2 and give your self a chances to adjust to the sounds, they can be over waming. Also, as my audiologist 20 years ago taught me that a cookie bite hearing loss can be a very difficult loss to fitt correctly.
To answer your questions about the actual db levels I cannot do so as I don’t know how to answer that question. You need to have a face to face talk with your audiologist. By the way your audiogram looks like what mine did about 20 years ago. And by the way a cookie bite hearing loss is a genetic hearing loss in almost every case.
Apparently I have a competent fitter, because my hearing is much as I remember it from when I didn’t have loss as measured by my music enjoyment. I really appreciate folks who educate the ignorant, as we’re trying to get up to speed as quickly as we can. But my flaw is as someone once told me, they said that when I drive up to a redlight I don’t just see red, yellow, or green. They correctly surmised that I envision relays, switches, and the automation that makes it work. Same is true about these new marvels.
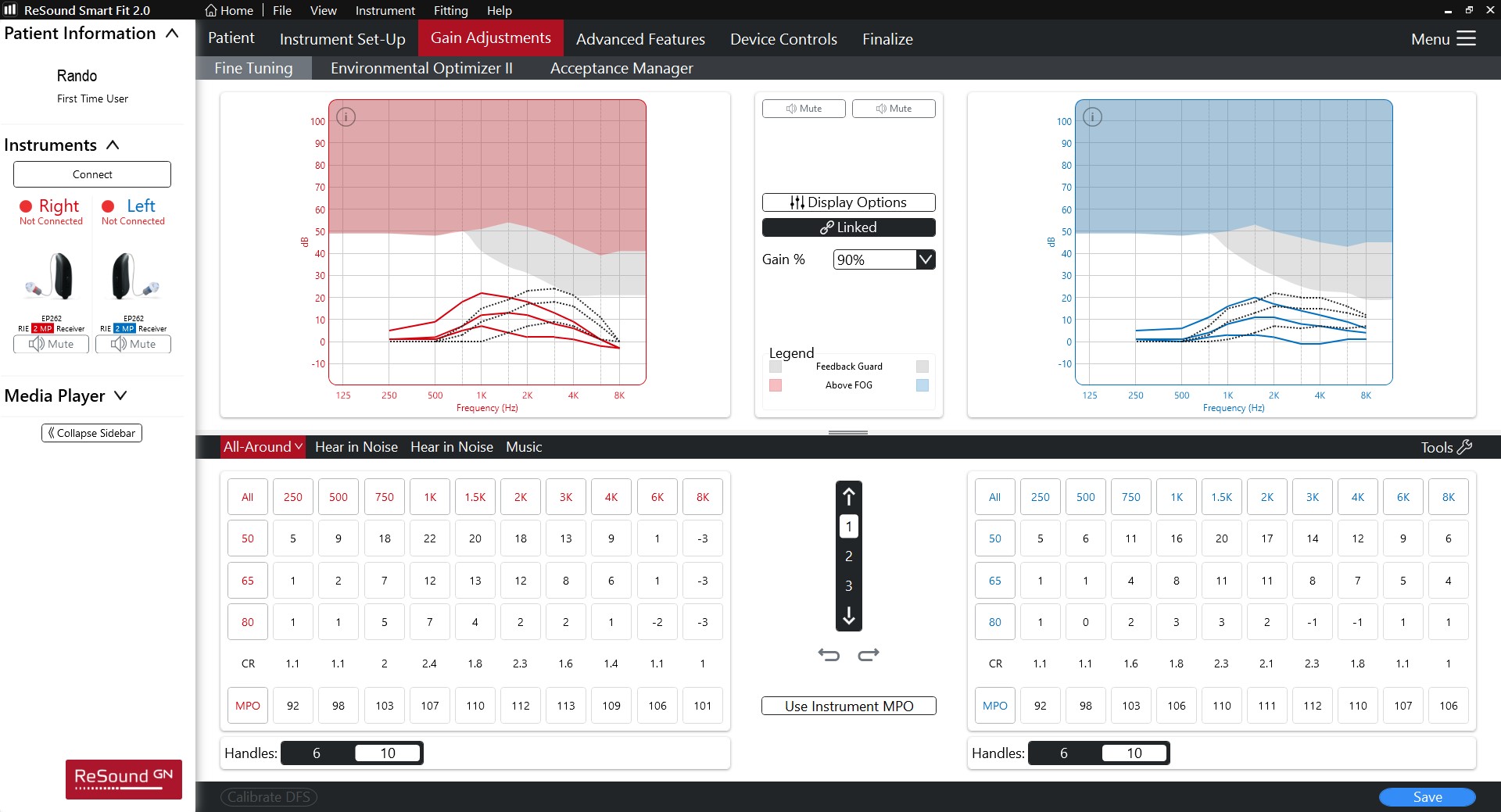
I’m including a pic of my REM tunings. I see there are 3 separate tuning levels, 50db, 65db, and 80db. I’m going to assume the boxes listed below are gain settings in db for each curve. So as a wild guess, I’d say that the maximum sound would be at the 80db curve in the right ear 1k range at 7db of gain. Total of 87db.
I know I don’t need to know this, but you’d be amazed that when you start learning to this level of detail what totally botched jobs you find from professionals supposedly in the know. Below the gain adjustments is CR, which I’m guessing is compression ratio. I have no clue what that is, or if those numbers are good or bad.
I am a retired IT professional, and I am a trained electronics technician/engineer, trained by the Navy. The Navy showed me that I am a natural born troubleshooter too. My present audiologist is a professor of audiology at the local university, and also an audiologist at the local VA clinic that I am using. I have actually set in and monitored his classes. But when it comes to my hearing I trust him to do what is right. Yes I have seen my REM results but my audiogram doesn’t tell the whole story of my hearing loss. My loss by the book calls for 85db receivers but in my reality my receivers are 105db receivers. Why you ask, because my audiologist and I have found that I have areas in my hearing that is much worse than the audiogram shows. Because I have areas that aren’t tested by the hearing tone test that is much worse, and these areas are in between the frequencies tested, and the results is that the frequencies not tested really determine my word recognition scores. So I have had an 18 month period of time that we have pushed my brain to accept louder sounds and the results has been improved speech understanding. And it also has lead me not becoming as tired as so many complain about from trying to understand conversations.
I’m not good at very detailed answers but I’ll try to give you a feel for what your asking. No, you don’t get 50 dB of gain added. You wouldn’t tolerate it. The goal is to get sounds audible. Say you have a 50 dB loss and there’s a 40 dB sound. If you add 20dB to it you’ll now be able to hear it.
Your dynamic range (range of loudness that you can hear) is now quite compromised. Whereas at one time you could hear sounds ranging from ~10dB to ~100dB, now it’s more like 50dB to 100dB. So the idea of hearing aids is to get more frequencies audible within the loudness range of what you can hear/tolerate.
All,
At my level of brain calcification I find it much harder to read and learn the highly technical papers. I’ve more or less become a visual learner, much to my chagrin! But, I really appreciate all the knowledgeable answers given.
At this point I’m simply trying to learn what all the jargon means. I don’t believe you can give an audiologist good feedback for tuning unless you know what the common issues are and how to describe them. For instance, 2 of the things I’ve noticed are fan noise and quiet sounds being (seemingly) unnaturally loud. Now I know that the sounds being loud is a part of the compression ratio, and excess ratio can become problematic. I can get used to that one, but the fan noises may need addressing. Once the noise reduction kicks in, fans cause 2 problems. One is a static like hiss, and the other is that at a slight distance from the fan, the noise reduction cycles on and off, resulting in a noticable pattern which could be annoying.
I think you’re better off describing whatever issues you’re having instead of stating what you think is happening.
You will likely adjust to certain sounds seeming too loud. If it’s too much, turn the volume down for now and report back to your audiologist.
Regarding the fan noises. Hard to say what is going on but the static like his sound MIGHT be "floor noise’ (the sound the hearing aid makes) It’s a low frequency noise and your low frequency hearing is pretty good. Your Audi can likely make the transition smoother if it’s too bothersome. Again, tell Audi what you’ve told us.
I never dictate to a professional, I’m just trying to better understand so I can use the right language so the tunings go smoother. I can’t tell you a good from bad hearing aid as my total ownership is one unit, and total time of hearing aid use is 7 days. I feel pretty confident the one I have is a good unit, and with the immense amout of tuning options I’m sure we can find a solution to anything that comes up.
Generally, that phenomenon many typically-hearing people are very familiar with of getting in the car in the morning and thinking, “Geeze, that radio is loud!” is a fatigue issue. As we are more fatigued throughout the day, listening becomes harder and turning up the volume often makes listening easier. Listening fatigue is compounded when you have hearing loss.
I think MDB already explained squishing the sound into your dynamic range well, and in regards to exactly what the presctiptive targets are doing it started out historically with the 1/3 gain rule and progressed over time to a fair bit of math to prescribe gain at each frequency based on your level and type of loss as well as the degree to which that frequency is important for speech and contibutes to loudness perception. So you can think of it as replacing roughly a 1/3rd of what you are missing but actually a bit more complex than that, but essentially trying to maximize audibility while managing a more limited dynamic range. It absolutely used to be the case that linear, analogue hearing aids could damaging your hearing and still sometimes causing damage can be something to worry about in with users who have profound loss and love powerful gain, despite wide dynamic range compression. However, we have good evidence that hearing aids appropriately fit to pediatric targets will not damage hearing over time and adult targets are significantly softer than pediatric targets. So unless you prefer your hearing aids to be set above pediatric targets, you don’t need to worry about increasing hearing loss from hearing aids.
But my regular refrain is: Don’t forget about the ear and the brain, it’s not just about adjusting the hearing aid. When you live with a hearing loss your brain gets used to a certain amount of auditory deprivation and when you replace the sound the brain re-adjusts over time, a little bit but not really like rehabing a muscle and being able to lift heavier weights over time. So it’s not always a great idea to think too hard about re-adjusting the hearing aid immediately (particularly downwards, reducing audibility), because it may well be that you don’t need to adjust the hearing aid at all, you just need to wait on the brain to adjust. However, we don’t have strong data on what the extent of that is and how long this adjustment takes. I would say anecdotally that there is, on average, significant adjustment within the first 4-6 weeks, and then to a lesser extent continued adjustment within the first few years, faster or slower in certain individuals. But adjustment is also different depending on the type of sound. In general, our perception of what is a “moderate” or “loud” volume is a lot more flexible than what our perception of “soft” is, which is heavily influenced by damage to the ear. That is, one of the jobs of the outter hair cells in the cochlea is the perception of soft sounds, and when those cells are dead we don’t really get soft perception back. So sounds that are moderate, like a lot of speech sounds, often sound too loud when you first get hearing aids and over time start to sound natural again, but sounds that were always truly soft, like the sound of your fingers rubbing against one another, are either audible or not through hearing aids and will never quite be perceived as soft as you remember. Those you either get used to (less like you get used to lifting heavy weights and more like you get used to a painting hanging on your wall) or you adjust them out. But by adjusting them out you may also lose critical soft sounds in the same frequency area, like soft consonants.
So if you are new, just focus on consistent wear for the next 4 weeks and then see what they sound like to you then, because it may be significantly different than they sound when you start out.
You have a way of adjusting for this, it’s called “Expansion” in SmartFit, as been mentioned give yourself some time to get used to these sounds, if over time it’s still an issue you can look there for adjustments.
Neville,
Outstanding explanation. I have read enough to agree with your synopsis 100%, and I fully intend to just wear the hearing aids until my next appointment. One thing I have going for me is mindset. So many choose the woe is me mentality, which actually slows progression. This is merely another step in the path. Adaptation is not a question, it will occur.
tenkan,
I’m trying to learn the jargon so I can at least follow the conversation. Today I’ve learned compression, and how the hearing aid logic works, and how a reduced dynamic range can change how I hear. And now A huge thank you to everyone assisting with my education. I had exactly zero exposure a week ago, but today I have a smidgen of knowledge. And now I have to go read about expansion!
No. WDRC is Wide Dynamic Range Compression. It often goes by “compression” Frequency compression is a whole different thing. Frequency compression is a type of Frequency shifting. Again, very different from “compression.”
Actually used the wrong word. Frequency lowering is the more general term I was looking for. It’s for losses like mine where the high frequency loss is too great to supply enough gain. Frequency lowering is unlikely to benefit you.
My father always told me i was ignorant when I messed up. I once saw him brutally reprimand someone for something really bad, he called him stupid. I asked him why I was ignorant, and the other guy was stupid. His reply has stuck with me to this day. He leaned down and softly said Son, ignorant doesn’t know. Stupid can’t learn. Then he told me I’d never be stupid because of my inquisitiveness. But I sure am ignorant in this subject field.
I’ll have to reread that article, see what I missed. I gather expansion is to reduce floor or minimum noises. If the compression is the part where quiet noises are amplified more than loud noises I think I understand that.
My dad was bluntly honest, but I never heard him call someone stupid or ignorant. He would always say do your homework, meaning go and figure it out. My day grew up during the depression, never officially got past the 8 grade. But left the farm went to work for a company as a janitor and rose to be the plant manager, learning every piece of equipment and every job along the way up. He was a natural born mathematician, he could do math problems in his head faster than any one could get the answer with a calculator. The must important thing he taught me was that I could do anything I set my mind on doing. I took that to the point of always proving people wrong when they said I couldn’t do something.
Frequency compression, frequency shifting and frequency lowering all fall into the same general technology. They can be implemented a little different but have similar results.
Might be helpful when you are researching hearing aids.
Stupid and ignorant are two totally different things.
Still learning, but making progress. Been reading and studying, but have some nonsensical questions at this point.
One question is, on the 50, 65, or 80 gain curves. If you hear a sound at around 57.5 db (exactly mid-point between the 50 and 65 db curves, does the hearing aid extrapolate the amplification or just use a linear computation like 50-57.5 gets the 50 db curve amplification, 57.6-72.5 db gets the 65 db amplification, and anything over 72.5db gets the 80 db amplification?
Frankly, I don’t see how they fit that much computing power into such a tiny case. I’m truly impressed.