Audigram Direct is a Phonak feature I have used quit a bit over the years. I’m in the process of buying new aids and thinking about switching brands.
How many of the other manufacturer’s offer the ability in their software to input tones to establish an audiogram?
About Audiogram Direct:
Test your client’s hearing directly through any hearing instrument fitted in Phonak Target, taking into account the properties of the individual ears and the chosen hearing instruments. It then provides a fast and accurate starting point for the fitting. AudiogramDirect ensures a more personalized pre-calculation, leading to enhanced spontaneous acceptance and less fine tuning efforts.
Additionally, it is very easy to select and compare diagnostic data obtained in different sessions without having to exit the fitting session. You are able to overlap two curves in the same view for easy comparison and showing the progression of the clients hearing loss over time, a feature that is extremely valuable in the counseling process.
More information: FSN_AudiogramDirect_V1.00_07-2011.pdf (598.5 KB)
Widex has this feature. For some reason, Oticon/Sonic have removed in-situ audiometry from the most recent versions of their apps. IIRC, Signia/Resound don’t have it.
Siemens/Signia and ReSound have had in-situ audiometry functions in their fitting software for many years.
1 Like
Thanks, Rasmus. Any idea why Oticon took away this feature?
It was just a matter of priorities. It’s on the list of nice things to have.
Here’s some info from Oticon. Does this suggest they have the same feature Phonak calls AudioGram Direct?
(Key Features)
1 Like
Yes. Also some background on the accuracy of in situ audiometry:
1 Like
Abram, if one uses in-situ, does that eliminate the need for REM?
Considering that in-situ is inaccurate, and especially unusable in cases of conductive hearing loss, I would always follow up in-situ based fittings with REMs, where possible.
I’m confused. I know nothing about audio measurements. . . But I’m being told in-situ is inaccurate because it doesn’t match another measurement technique. Yet it seems in that study the clients were not consulted. Frankly I don’t think the clients care what the numbers are or if they are “inaccurate”. The client is after an outcome where they can hear.
The conventional hearing test and rem depend on the equipment being properly calibrated. So is everything always properly calibrated? What happens when they aren’t?
During an in-situ test who cares what calibration is. The aid generates a tone and asks the client, can you hear me now? Can you hear me now? Can you hear me now? This is how much noise I’m going to make at this frequency, can you hear it? Peculiarities of the aid, receiver, and ear canal all in place and the client asked if they can hear.
Yet this is supposed to be less accurate.
School me on this.
1 Like
In-situ can be accurate, Widex has used the method (Sensogram) for years to establish in situ gain adjustment. It’s simply not transferable, which is often the basis for such studies - which involve comparisons of efficacy.
However, within the closed loop of a single fitting, the gain adjustment from the transfer function generated by the in-situ measurement works - and you can check the result with a separate R.E.M. However, the gain will not necessarily reach the full R.E.M. target, simply because the manufacturer wants the hearing instruments to sound good on the first fit, rather that the potentially ‘harsh’ full prescription.
1 Like
It would be a fascinating run in-situ and then choose NAL-NL2 over the manf’s own fitting rationale in the programming software, and then verify a NAL-NL2 target. My guess is even then the REMs would be off … not sure such a study has been done. I performed in-situ with Widex/Oticon/Phonak in the past and was never happy with the resulting REMs, but it’s been a while, and I can’t recall whether NAL rationales were available or whether I selected them.
1 Like
In theory… In practice, I’m not sure.
I’m very new bee and a HA user.
I use PHONAK AUDEO serie and SIEMENS PURE BINAX, both RIC type.
Considering PHONAK AUDEO, I have 2 pairs;
S SMART III-312 xP
Q70-312 xP
If I interchange the receivers (both are xP) from S SMART with Q70, my final hearing sensibility is different. I guess it is due the intrinsic difference in receivers production.
So when a ha user measures using in-situ or audiogram direct … I think that this process consider the particular difference between RIC pair or even HA deviation.
Just my humble thought.
Sincerely
I raise this topic from the grave, here is the topic from 2017. But I’m just wondering what the situation is now with the AudiogramDirect option.
Has anyone now worked with the new Paradise series of hearing aids to see how effective this IN-SITU option will be compared to the one done according to the audiogram and of course according to the REM measurement.
Could the measurement now be carried out with the installation of noise shields to eliminate external noise. Because new hearing aids do not need a wired connection.
in situ and audiogram direct is same…
REM is different
onl audiologist can perform REM with costly equipment
I figured it out.
We do the audiogram in a cabin that is soundproof and we raise our hand when we hear the slightest quiet sound and it is then marked on the chart.
And “In-situ” is when we do it with hearing aids.
REM is a measurement of hearing to determine if a hearing aid is delivering sound as prescribed by an audiogram. The hearing aid may measure the volume differently, or perhaps the cause of the insufficient or excessively amplified sound may be in the mold or uneven channels in the ear. I read that somewhere on some forum.
In-situ should be the most accurate measurement, because we do the same thing we do when we make an audiogram. The chart may not be the same as in the Audiogram.
And when we go to REM, it will look at the audiogram to see if the hearing aid is delivering the same sound. Whether I understood correctly or not, correct me if I am wrong. Isn’t REM wrong then? The equipment we use for Audiogram will probably not be calibrated in the same way as the hearing aid.
wrong
REM is to find prescriptive target is correct
let say you wear dome so gain is to give 20 db
but actually its giving 15 db even though software show 20 to compensate REM will add another 5db …
Reviving this topic once again.
For the past 10 years I have always relied on the Audiogram done by competent audiologists. I have a record of them over the years and can see my hearing decline gradually as I age (and hopefully not because of bad hearing protection habits).
And, for my last three annual “checkups” I was able to benefit from REM adjustments to my HAs (currently M90-R). My last Audiogram was 14 months ago. Before planning to travel 2 hours to my audiologist again I spent some time (quite a lot of time) experimenting with AudiogramDirect (Target’s in-situ hearing test software). Here is the final result - the grey is the 14 month old Audiogram and the red is my right ear AudiogramDirect result…
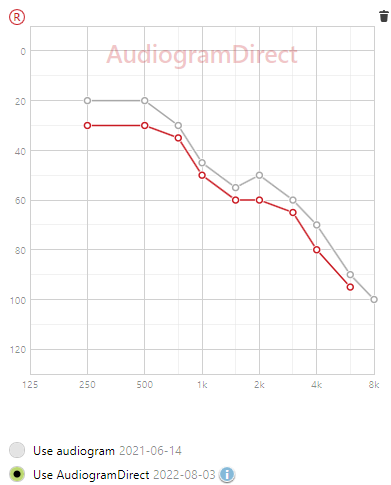
The difference could be due purely to a 14 month decline in my hearing, but I doubt it (based on my 10 year trend pattern of decline). And, after applying the results of the AudiogramDirect my hearing is greatly improved across the range (not surprisingly). So, I don’t yet have the benefit of REM on top of these AudiogramDirect results but my hearing is currently about as good as I can ever remember (i.e. since before 10 years ago).
Could it be that conducting one’s own AudiogramDirect is “more accurate” than the audiologist’s Audiogram? Note: I probably ran the AudiogramDirect tests over 20 times overall to get them as exact as I could, in a very quiet room. I tried various levels of “I can hear that”, applied the results, and tested the sound of the HAs over a few days. Each time going back and adjusting up or down the amount to which “I can hear that”. The happy medium, for me, was when I could just barely hear “something” then went another step louder to where “I know I can hear that” but softer than “I definitely hear that very clearly” - if that makes sense.
I’m just offering my personal experience at this and hope it helps someone else. It’s definitely worth a shot and I think I’ve gotten my HAs “better” (for me) than what my various audiologists have arrived at in the past (no knock on them - they are very good at what they do but, I think, appropriately err on the side of being a little conservative.)
2 Likes