Harvey Dillon’s 2012 book Hearing Aids has a great and comprehensive review of venting (thanks to MDB for the tip that Dillon’s book might be helpful in better understanding HA’s). To tell whether you’re getting any discernible occlusion, he suggests the simple “ah, ee, oo” vowel test. With HA’s out, you can perform the test with and without fingers in your ears and try it with your HA’s on also. If “ee” and “oo” sound louder than “ah,” you’re getting occlusion.
I suggest anyone deeply interested in this stuff buy a copy of Dillon’s book (to make up for my fair use of his info here!).
He says “If a patient needs a gain of 0 dB below some frequency, no electronics can compete with the low distortion, flat frequency response that a vent can provide.” Reason for not having venting “high frequency gain cannot be achieved if vent is use” or “important for patient to have benefits of directivity in low frequencies.” (see my previous posts on speech clarity, directionality, and noise control above with more occluding fit).
Note in all these figures how close a 1 mm vent size is to a fully occluded fitting (my experience described in posts above).
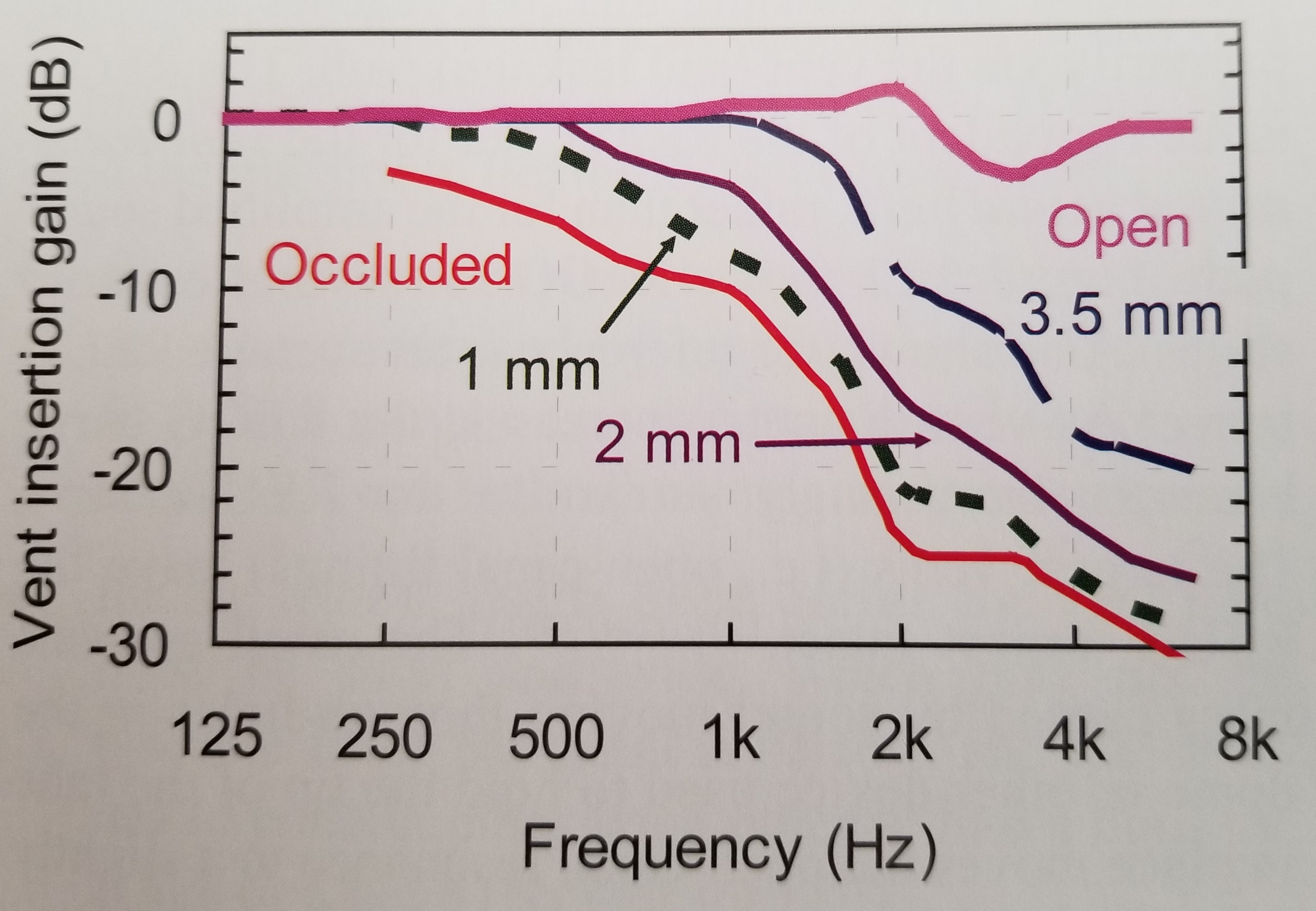
Diagram 5.11 on page 137 shows the relative loss of gain from HA amplification as a function of frequency for various degrees of venting from open to occluded. Note that if you have good low frequency hearing, the loss of gain from the HA’s won’t matter as it will be compensated by low-frequency sound coming in through vents. The loss matters when your low frequency hearing is not good and is in need of added gain.
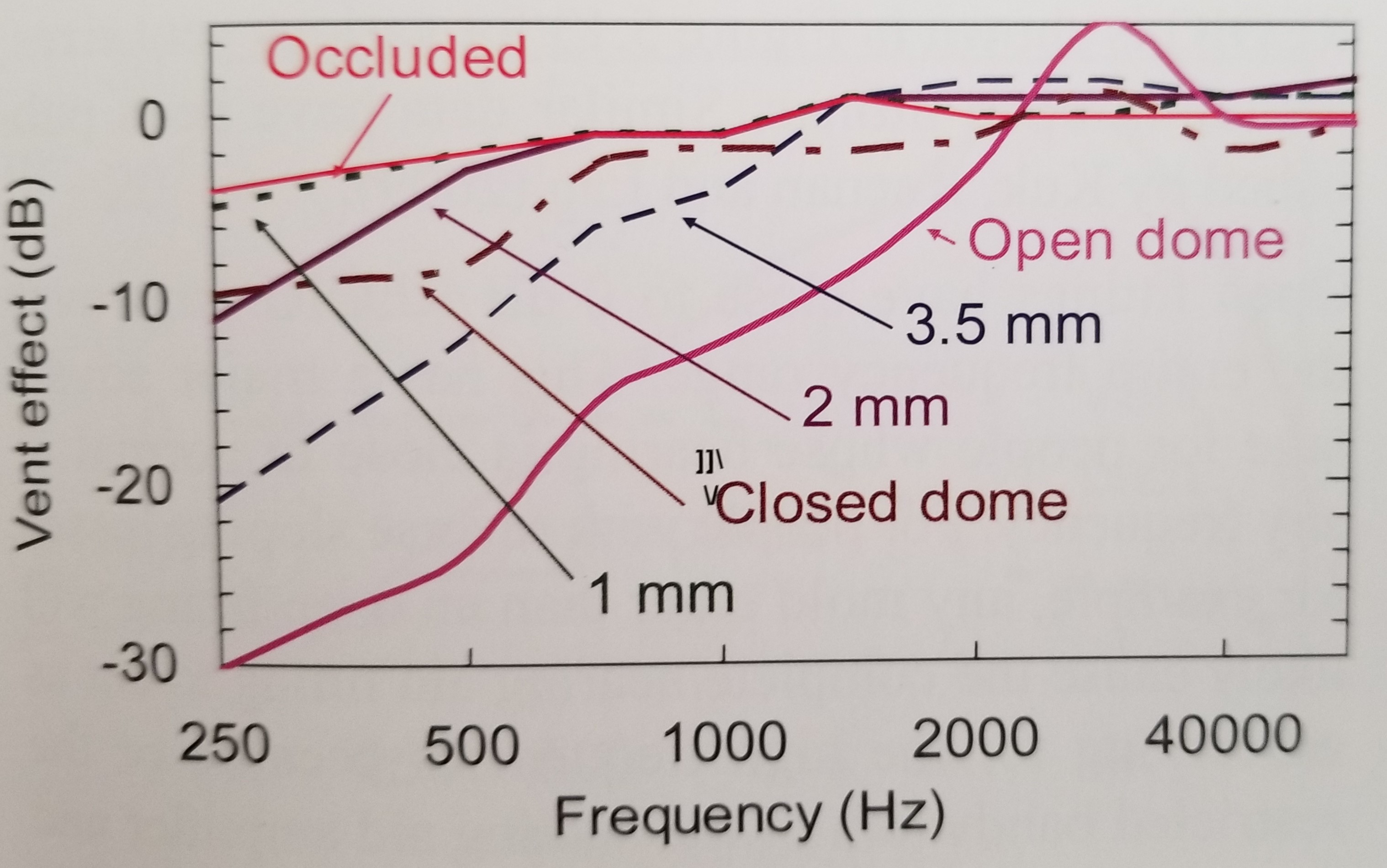
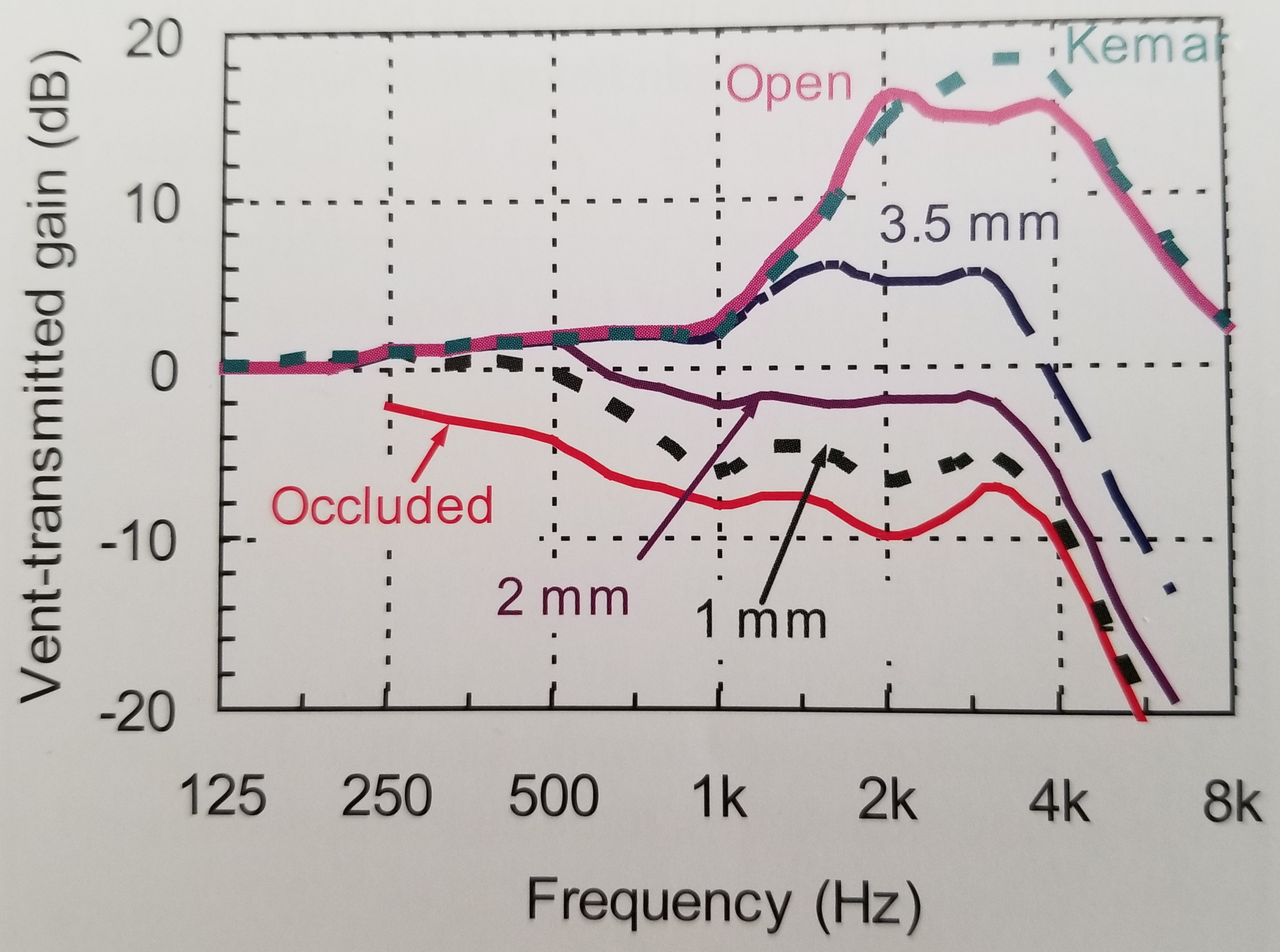
Figure 5.12 shows the relative gain of vent-transmitted sound as a function of frequency for various vent sizes from open to occluded. Note that an occluded fitting shows relatively little blocking at low frequencies as compared to high frequencies, which has been my experience (exact definition of occlusion is not given).
Figure 5.13 essentially shows the earplug effect. If your HA’s are turned off, with different degrees of venting as a function of frequency, what sort of gain loss will you experience relative to your unaided hearing? The figure shows the earplug effect of occlusion vs. a very open fitting.
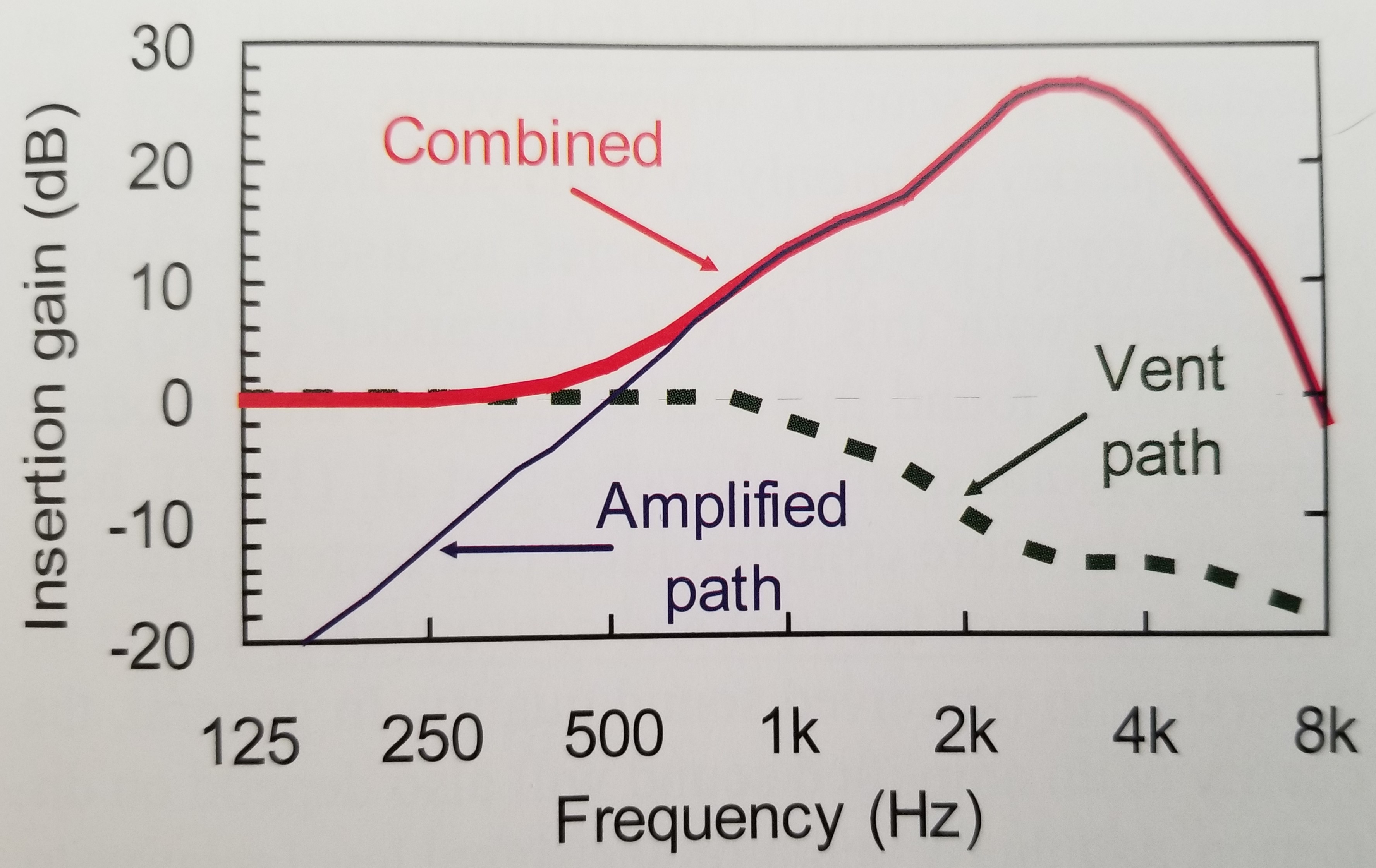
Figure 5.15 shows how gain through a vent path and gain through an amplified path (your HA’s) combine to produce the overall gain that you hear in your ears. Did not see details in text on size of vent used for illustration (a reference is cited in the text for figure) - based on Fig. 5.11 shown above and loss of gain depicted in Fig. 5.15 for amplified gain at low frequencies, the venting depicted in Fig. 5.15 is probably about a 2 mm vent. Dillon says when any one path has more than 10 dB of gain over the other, that path is the dominant and effective path.
Dillon does mention two other possible drawbacks for a more occluding fitting. Increased moisture in the ear and a greater chance of ear infection - but he doesn’t give statistics on the latter. Seems more of a feeling from experience than scientific data.

 I was confident though that it would be a good place to obtain a lot of knowledge in organized fashion. Textbooks are often out of date, but they make great resources from which to obtain background knowledge, especially in fields one is new to.
I was confident though that it would be a good place to obtain a lot of knowledge in organized fashion. Textbooks are often out of date, but they make great resources from which to obtain background knowledge, especially in fields one is new to.