
I’d probably just try the quick and dirty of replacing the vented click sleeve with the closed click sleeve and see what you think. If I’m remembering correctly, this is all about sound quality. Programming changes are likely to be minor. If you end up liking how it sounds better, then consider getting reprogrammed and new REM. Whether to use one or both ears with click sleeves–again try it and see what you think.
2 Likes
Seems to me that just switching them would be asking for a failure. But, perhaps the issues I see are not significant. My expectation is that low frequency gain will have to be reduced, and the own voice program redone to keep it sounding right to me. And the other, perhaps less significant issue is that more gain may be possible without feedback, assuming feedback is currently limiting gain at certain frequencies.
Here is something I did until my molds came in. I used silicon earplug putty behind my domes. it comes in a quarter sized hunk you roll in your hand then put in your ears. They are made by Pro-Optic. You can stop feedback by doing this until you get adjusted. you can also see if it sounds better. You pick up a lot more bass this way. Most drugstores have it.

1 Like
I hadn’t considered the OVP aspect. I’m prone to quick and dirty approaches so I’d still probably try it the way I mentioned, but it’s certainly fine to do a more careful approach.
I ran the simulations with closed and the current vented fittings, and on a quick look the differences are no more than 1 dB, so essentially inaudible. We’ll see what the fitter says. Looks like it would not be a disaster if she just gave me the closed sleeves to try.
I’m still thinking it will change my own voice perception, and I see no way to simulate that in the software.
Harvey Dillon’s 2012 book Hearing Aids has a great and comprehensive review of venting (thanks to MDB for the tip that Dillon’s book might be helpful in better understanding HA’s). To tell whether you’re getting any discernible occlusion, he suggests the simple “ah, ee, oo” vowel test. With HA’s out, you can perform the test with and without fingers in your ears and try it with your HA’s on also. If “ee” and “oo” sound louder than “ah,” you’re getting occlusion.
I suggest anyone deeply interested in this stuff buy a copy of Dillon’s book (to make up for my fair use of his info here!).
He says “If a patient needs a gain of 0 dB below some frequency, no electronics can compete with the low distortion, flat frequency response that a vent can provide.” Reason for not having venting “high frequency gain cannot be achieved if vent is use” or “important for patient to have benefits of directivity in low frequencies.” (see my previous posts on speech clarity, directionality, and noise control above with more occluding fit).
Note in all these figures how close a 1 mm vent size is to a fully occluded fitting (my experience described in posts above).
Diagram 5.11 on page 137 shows the relative loss of gain from HA amplification as a function of frequency for various degrees of venting from open to occluded. Note that if you have good low frequency hearing, the loss of gain from the HA’s won’t matter as it will be compensated by low-frequency sound coming in through vents. The loss matters when your low frequency hearing is not good and is in need of added gain.
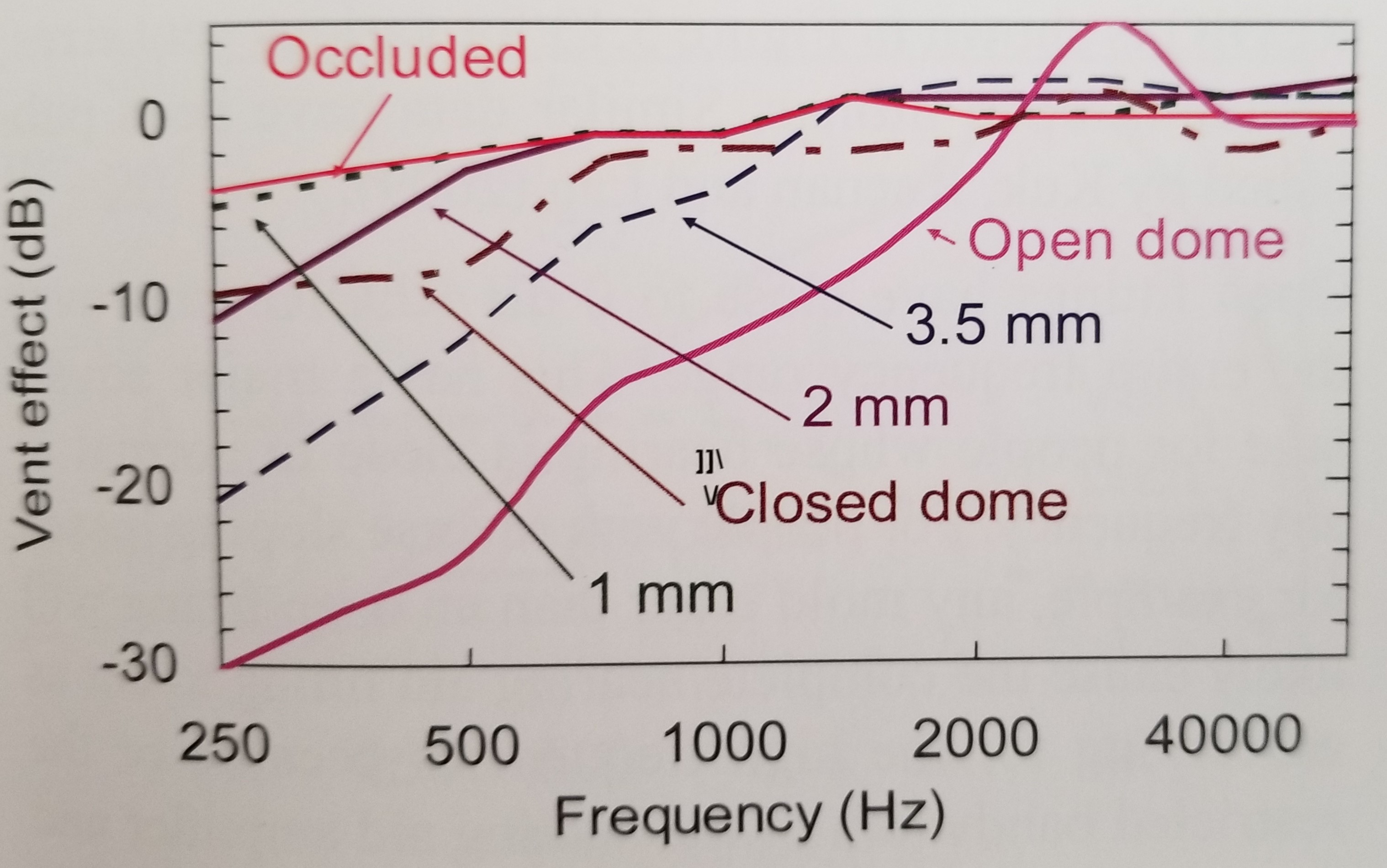
Figure 5.12 shows the relative gain of vent-transmitted sound as a function of frequency for various vent sizes from open to occluded. Note that an occluded fitting shows relatively little blocking at low frequencies as compared to high frequencies, which has been my experience (exact definition of occlusion is not given).
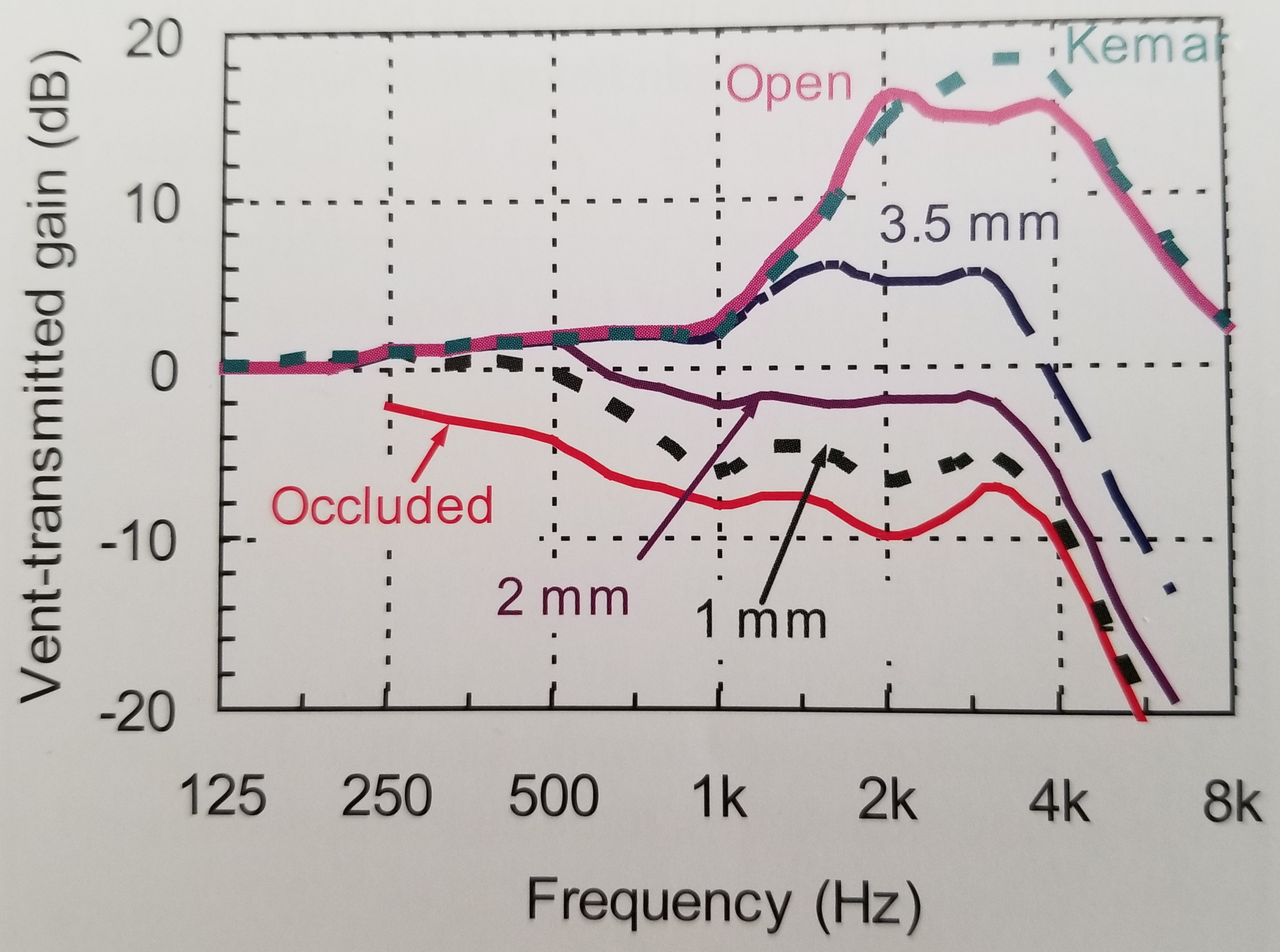
Figure 5.13 essentially shows the earplug effect. If your HA’s are turned off, with different degrees of venting as a function of frequency, what sort of gain loss will you experience relative to your unaided hearing? The figure shows the earplug effect of occlusion vs. a very open fitting.
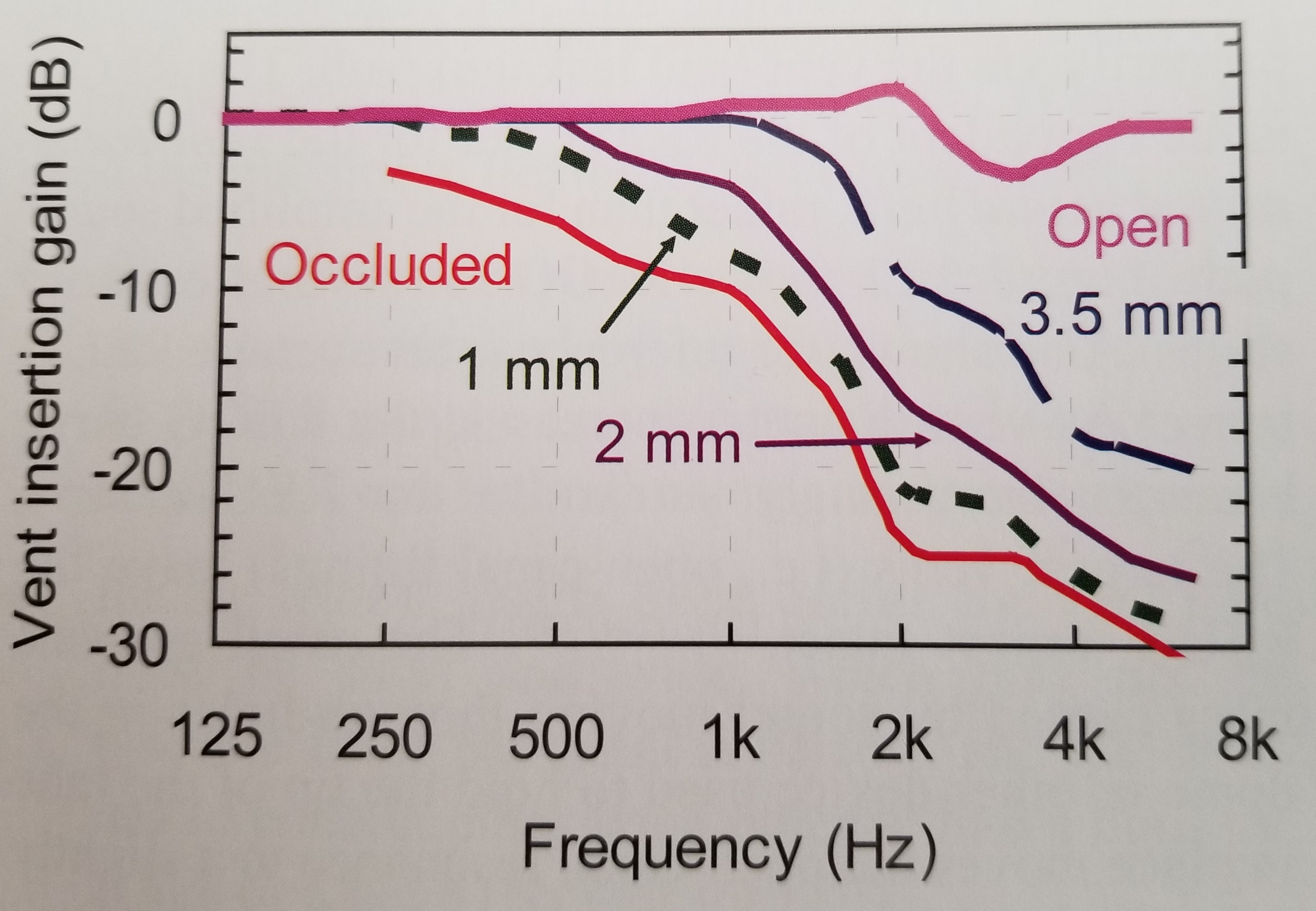
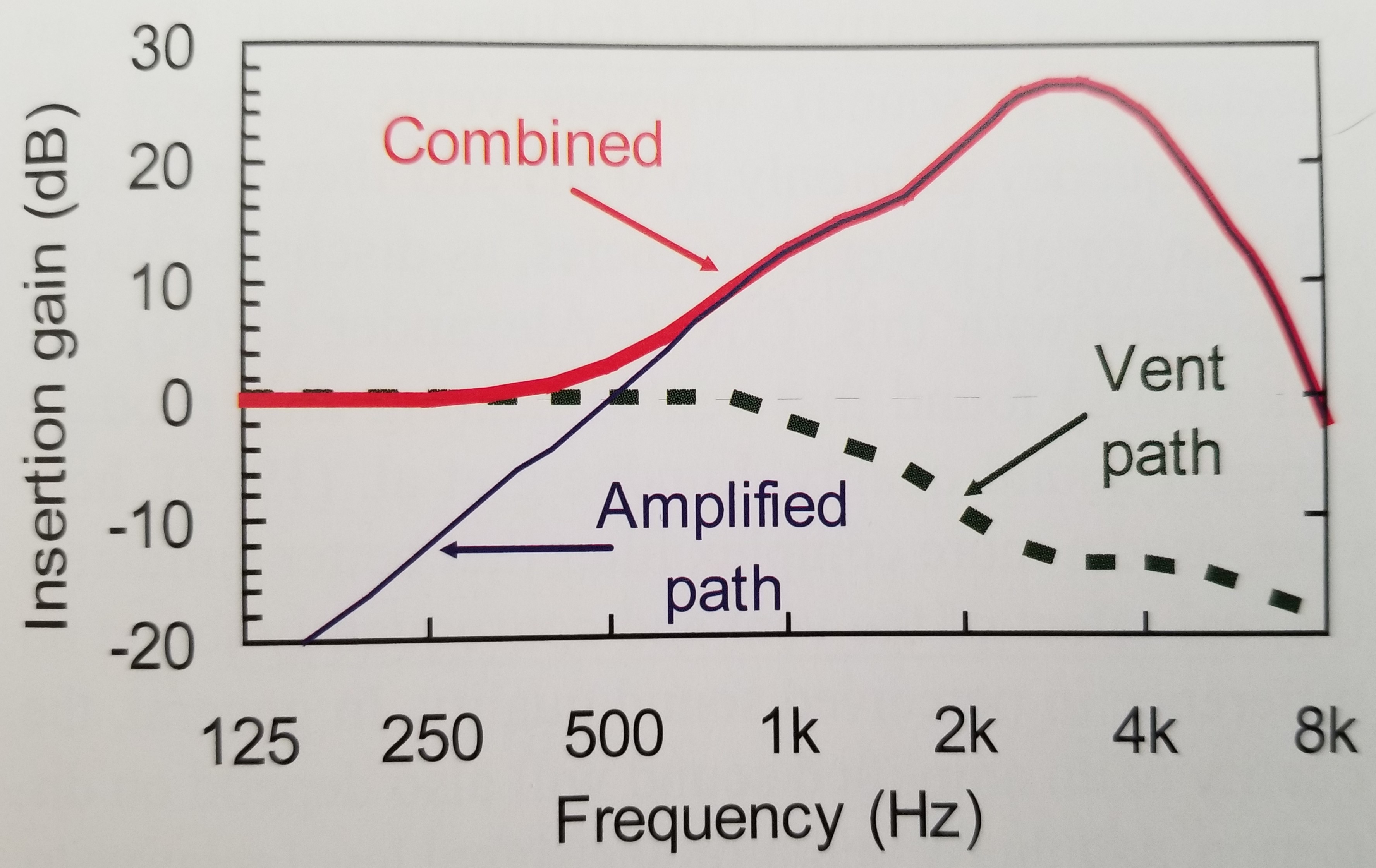
Figure 5.15 shows how gain through a vent path and gain through an amplified path (your HA’s) combine to produce the overall gain that you hear in your ears. Did not see details in text on size of vent used for illustration (a reference is cited in the text for figure) - based on Fig. 5.11 shown above and loss of gain depicted in Fig. 5.15 for amplified gain at low frequencies, the venting depicted in Fig. 5.15 is probably about a 2 mm vent. Dillon says when any one path has more than 10 dB of gain over the other, that path is the dominant and effective path.
Dillon does mention two other possible drawbacks for a more occluding fitting. Increased moisture in the ear and a greater chance of ear infection - but he doesn’t give statistics on the latter. Seems more of a feeling from experience than scientific data.
2 Likes
I will keep that in mind. Looks like it would be a good way to make well fitted ear plugs too.
Thanks for the detailed post. It is going to take me a while to digest it. Reminds me of when I designed and built my tuned vent subwoofer…
It is not that common that closed domes are truly occluding the way custom products are, regardless of what their venting is supposed to be. I’d agree with MDB–just pop the closed domes/sleeves in your ears and turn the hearing aids off. If you are bothered by the sound of your own voice with the closed domes and the devices off, you will not tolerate closed domes even with OVP. If you sound fine to yourself, reprogram to closed.
1 Like
If you’re really into understanding how HA’s work, a used copy of Dillon (~$60 thru Amazon or other used booksellers) might be worth it. There’s more on venting that I didn’t post here for fear of violating copyright. The book is very thorough - a lot of material is obsolete - but the important thing is the information is all highly organized. Hearing Tracker has lots of great information, too, but it’s all scattered pretty much here and there whereas Dillon gives HA function a very systematic exposition. Thanks to MDB, again, for the recommendation, Especially after reading the section on venting, I felt it was worth the expense but probably not worth it to anyone unless they really want more in-depth explanation for DIY. My recommendation might be premature, too - I’m only about 90 pages into a text that’s 536 pages long before you hit the references and index, 608 pages total.
Another neat thing that I learned from Dillon - don’t know if most practioners give it as much weight as he does - is the concept of critical distance - the radius at which reverbant sound in a room begins to dominate over direct sound from the source and consequently muck up speech intelligibility more and more - and the idea that beyond that distance directional microphones on HA’s or a remote microphone may gradually become more and more helpful in increasing the SNR by allowing better detection of direct sound over reverberation/noise. So by going with a more occluding fitting, hopefully I’m helping both HA directionality and external noise suppression to enlarge my “critical” distance (Dillon emphasizes it’s not a hard black & white boundary, just the point at which nondirect sounds (and noise) begin to dominate more and more as you go further and further away from desired source.
Hey, what’s select a vent?
There are different styles of Select-a-Vent depending on the mold manufacturer or supplementary supplier.
Mine are like the above except there is a mix of mini and standard sizes on the same tree.
Westone has a rather different, shorter vent insert (see bottom of Westone page).
https://www.westone.com/store/hearing_health_care/index.php/venting
The acoustic and limiting properties of a vent increase as its bore size decreases and its length increases, so the narrowest and longest vent bore path in a mold predominates if it’s just one bore with varying diameter along its length (Dillon, 2012 Hearing Aids book).
1 Like
https://www.westone.com/store/hearing_health_care/select-a-vent-sav
Do these with with phonak hearing aids b90 behind the ear?
I don’t know - one of the providers or much more knowledgeable folks on the forum might know. I just asked my audi to have custom molds made by ReSound, I told her I wanted Select-A-Vent with the vent holes in the molds. So when I got the silicone molds back, they had ~4-5 mm vent holes curving a bit with the shape of my ear canal and she gave me several trees of “standard” and “mini” inserts that fit the holes in the molds (the right and left mold are different sizes and have different size vent hole diameters), plug them up, and only offer the smaller diameter bores of various sizes in the inserts. By using them, I am deliberating making the venting more occlusive, which has both possible advantages and disadvantages, depending on your hearing environment and what you want to get out of your hearing in a particular situation - but it’s like cleaning your hearing aids or changing the batteries - changing the vents, once you’ve found a size you like, is not something you probably want to do too often and it would be best done in a safe, clean environment as the inserts are dang little, very translucent, and easy to loose if you’re not careful.
1 Like
Jim, Thanks for always crediting your sources. I’m glad my suggestion is proving interesting and helpful. Pretty funny that I haven’t read it.  I was confident though that it would be a good place to obtain a lot of knowledge in organized fashion. Textbooks are often out of date, but they make great resources from which to obtain background knowledge, especially in fields one is new to.
I was confident though that it would be a good place to obtain a lot of knowledge in organized fashion. Textbooks are often out of date, but they make great resources from which to obtain background knowledge, especially in fields one is new to.
Well I have run simulations in Connexx for vented sleeves, closed sleeves, and custom mold with a 2.5 mm (Connexx recommended size) vent. The differences are trival. Based on the very informative charts posted above by Jim, I was expecting significant differences. I think I must be reading the numbers from Connexx wrong…
In any case I went for my Costco appointment yesterday, and the fitter was very accommodating. First she did the gain test for feedback. It showed my current setup was marginal in the right ear for feedback, and problematic in my left ear. It validated what I was hearing. She then tried the closed vents and tested again for feedback. The improvements were quite modest which was enough for the right ear, but not for the left ear. She said she was reluctant to save the gain test as it would then take over and limit what gain she could apply in the REM process. So, she manually recorded the problem areas, and said she would make manual adjustments.
Next she did the REM and adjustments with a closed sleeve in my left ear, and a vented sleeve in the right. That was saved in Program 1. After that she used a closed sleeve in both ears and saved the REM adjustments in Program 2. I asked her about the need to redo the Own Voice Program again, but she said it was not necessary.
So now I have three weeks to evaluate what I like. My first impression was not great with a closed left and vented right. Somehow everything seemed significantly louder, kind of like when I first got hearing aids. Today I tried the closed sleeves in both ears and that seemed better. Still seems a bit loud so something must have changed in the REM adjustments.
She thought I should think about a custom mold with a vent for my left ear. So I am wondering what advantages that might have? I suspect the vent feedback may not even be as good as the closed sleeves. Any thoughts on that appreciated. The cost of the mold option does not concern me. So far I find the closed click sleeves fairly comfortable and not intrusive. My plan is to mainly go with the closed click sleeves until the next appointment to see how I adjust to that fitting.
2 Likes
For most fits that I’ve tried I’m well below the feedback region in my prescribed fits except when I’ve had DSL5-Adult and I don’t have any REM adjustments applied. So I could be free and easy with feedback tests and I always found the potential for feedback that showed up pretty much matched my sense of “openess” vs. occlusion and since a feedback test was a lot easier to do and reach a visibly comparable graphical conclusion very quickly, I found that the best way to judge how much occlusion I was getting, then see over a longer time if I liked the quality of hearing that went with it. I do find custom molds made of ~hard silicone very comfortable and mine probably go just up into the region between the first and second bends of the ear canal. They are each about 1.5 cm deep without allowing for the slight curvature of the mold past the first bend.
On page 136 of the 2012 ed. Hearing Aids book, Dillon wryly comments that on molds fitted with selectable vents, you really only get 2 to 3 different distinct options for venting:
“It will commonly be the case that the inserts with the largest and second largest holes will have almost identical effects (because of the total vent mass is dominated by the vent tube <of the mold>), and the inserts with the smallest and second smallest holes will have similar effects to each other (because the natural leakage dominates the venting effect). The insert system is nevertheless worthwhile in that it offers an easy way to obtain two or maybe three effectively different vents.” (he then gives some further conditions, i.e., minimizing mold leakage for best use of small-holed inserts or having a short, wide hole in the mold if you plan to use large inserts, to get the best possible results).
Since I’m using very occlusive inserts in my molds, I found his further comments on p.144 interesting. He says occluded molds generate additional low frequency sound during chewing and walking. For chewing, I only notice the additional sound if I’m eating something crunchy. I have no annoying pressure sensation chewing as I did when trying tulip domes or oversized power domes. For walking, I only notice any foot sound if I am wearing over-the-ear headphones but not at all otherwise. My theory is that the earcups of the headphones are so tight-fitting and spring-loaded that any vibrational movement from walking causes air pressure inside the cups on the molds to wax and wane. Wearing the same headphones with open domes, I noticed little or no foot padding sensation as I walked. Further along in the same paragraph, Dillon says that lack of ventilation and increase in moisture because of an occluded fit may increase the likelihood of external ear infection - but then that would be something everyone with very severe or profound hearing loss and an occluded fit faces the possibility of.
p.145 Dillon has several tables of gain possible before feedback vs. frequency for different degrees of venting and the tables basically show that with a more occluding fit, you can get a lot more gain before you risk feedback.
I guess for me my two ear canals are different in size and shape and it was very hard to find a standard size dome that fit either well, given the degree of occlusion that I wanted, and was comfortable to wear at the same time. The molds give me some control over the degree of occlusion, fit very tightly with little leakage, and are very comfortable to wear. So since we’re all a bit different, everybody’s going to have somewhat different results
Thank you for the comments. I am going to give these closed sleeves a try for a while and see what happens. Second day with the sleeves and they are not too bad. Second day with the sleeves and they are not too bad. The custom molds may be next if these do not work out.
I’ve found a paradox of having a more occlusive fitting and being able to turn up gain while wearing your HA’s is that it’s easier to have the HA’s generate feedback on their own when you take them out. While they’re in your ears, sound generated by the receivers looping back to the external mics is very well blocked by tight-fitting molds having little or no venting, so the gain can really be cranked up and the feedback management algorithm made very mild.
However, when I take the HA’s out and the receivers come near some reflective surface and there’s nothing to block the sound from the receivers traveling through the open air to the external mics, it’s like, “Wow! Look out!” Since I have moderately strong to severe high frequency loss, it’s hard for me to hear that feedback is occurring with the HA’s out of my ears. I now turn the amplification off (but not the HA’s) in the smartphone app before I remove my HA’s (and an odd Resound Quattro behavior is that if you then turn one HA completely off via its switch, the amplification of the other HA gets turned back on (crazy!) - so I use the app again to turn off the amplification before shutting the last HA down as otherwise the receiver waving around in my hands can generate feedback as I go to operate the HA body On/Off switch). Just worried I’ll damage my receivers by too much really out-of-control feedback if I’m not careful.
Further note on the walking sound: it only happens on a very hard surface like an asphalt road. Don’t notice it at the gym walking on the much softer, more pliant belt surface of a treadmill. And it does have something to do with the headphone frame as I can increase or decrease the footpad sound by the way that I angle the headphone headband on my head, tilting the headband forward or back relative to the position of the earcups lessens the mild thumping sound relative to having the headband straight over the earcups.
Streaming via my Phone Clip+ directly to the Quattro’s eliminates the headphone footpadding problem but I don’t get the benefits of noise-cancellation/noise-blocking that I do for other bothersome really loud noises when I wear my over-the-ear noise cancelling headphones and stream to them instead of directly to the HA’S. Perhaps I should try streaming to my HA’s via the PC+ while wearing the noise-cancelling headphones and see what happens to the footpadding sound on hard asphalt…
Edit_Update: Streaming directly to my HA’s while wearing the headphones or gun muffs to block out extraneous loud noise (e.g, 10 motorcycles in a “gang” zooming up a nearby major street!) doesn’t work to block out frame vibrations from any over-the-ear device I’ve tried. If I hold part of the frame of the over-the-ear noise blocking device while I walk, that reduces the footpadding sound on hard asphalt that shows up as a result of my occluded fit. So either changing vent inserts for a walk to something less occluding or finding an over-the-ear frame that doesn’t have springiness or rattle from walking is likely to be required to solve my walking on hard surfaces with a Closed Fit problem. Or just not resume streaming until all the motorcycles, helicopter, or whatever has passed by and not wearing any over-the-ear device while streaming directly to my HA’s might do it, too.
This has been an interesting feed I am a newbie
I only have one ear due to birth defect and my hearing in my ear is bad I use a RIC with earmold and reading about the pressure is interesting…other day was running late and just grabbed my aid and put it in. All day my ear felt strange clogged could not clear that evening took aid out and noticed that my vent was clogged on my mold with wax Cleaned out and put back in everything felt great and normal again