
You could make screen prints of “all” your settings.
2 Likes
Yes, the RECD and REUG tabs allow for manual input. After the input you can choose between the input values or estimated values. The RECD are estimated during the feedback test. No idea on what they base the estimation of the REUG. Hopefully based on some empirical data taken from large groups. 
Do we have to fill in these? Are these values important?
If you don’t have them, you’ll need to go with the provided estimations. I got those values (Real Ear Unaided Gain) from the Oticon Genie software, when I hooked up a pair of HA’s that I was testing. You could try your audiologist at the hospital. They also measure those values, when you go for their confirmation of correctness of your HA’s. (Not necessarily new HA’s! But this step is a must if you want the insurance to pay their share.)
My audiologist did a REM, but the hearing aid is not ok (yet).
My audi is nice and is willing to provide me with any data that I want or need in order to tweak the programming of my hearing aids at home.
What is the absolute minimum data I need from my audi to maintain REM calibration for self-programming? I know that I need the REUG data for sure. My audi didn’t know how to retrieve the RECD data from Otosuite.
I have a few other related questions:
-
Is there a specific way I should ask REMs to be performed, i.e. NAL-NL2 target, manufacturer’s module, etc.? Is there a specific way that will yield better results for my purposes, i.e. preserving the REM calibration so I can do further tweaking at home?
-
Am I understanding correctly that once I have this data, I theoretically don’t have to run REMs again for every change that doesn’t involve changing the acoustics? That is my ultimate goal.
Any tweaking you do after REM is moving off of prescription targets. The reason you want to have REM completed in the first place is to ensure you are at least meeting prescriptive targets and not just being dramatically underfit at one or all frequencies as is common with hearing aids that don’t have REM completed. It also ensures that the hearing aids are taking into acount your individual ear canal acoustics as well as the venting/coupling acoustics.
Prescriptive targets are the best AVERAGE settings we have come up with so far. Not everyone is average and so things may need to be tweaked, but keep in mind that the auditory system has often been deprived for a long time in advance of hearing aids and takes some time to re-adjust. Loud and moderate volume perception is also quite flexible (to a point), so things that sound loud at first may not sound loud over time. So you want to make sure you’re meeting prescriptive targets to start and then make sure you are giving your brain that time to adjust before deviating too far off of target, particularly by turning things DOWN. Tweak upwards at will with the exception of the MPO, which you should leave alone after the audiologist sets it.
Just save the entire fitting so that you can roll back to it if necessary.
If you’re in Oticon hearing aids and your audiologist is friendly, you could ask for a program set to NAL-NL2 targets AND a program set to DSL 5.0 Adult targets, and then you’d have both and could see what you liked.
3 Likes
If one has a copy of the REM showing the target curves for Loud, Moderate & Soft, how can a DIY’er use this info in adjusting the gain of the hearing aid? I can see that the REM is showing REAG (y-axis) and Frequency (x-axis)
-
How does one correlate the numbers in REM with the manufacturers fitting program (e.g. Phonak Target)? What setting in Gain & MPO (e.g. output, 2cc etc) should be displayed in the Phonak program in order to see the correlation between the REAG numbers in REM?
-
Does one have to apply the REM results to all the program settings of the hearing aid? As an example Phonak Brio has 9 automatic programs (Quiet, Noise, Loud noise, etc). Do we need to adjust each of these automatic programs one by one according to REM results?
Thank you!
For some reason the post above is a reply to one of my previous posts, but I think @Neville is more suited to answer these questions so I’m tagging him here for awareness.
I’m not really clear what is being asked. If one has their REM results and it looks like they are off target in some way they could adjust blind in the areas that they are off target, but the manufacturer numbers don’t correlate as closely as one might like. If one just has a print out of the desired targets… There’s nothing you can do with that because you have no idea where the manufacturer has started you out.
Thanks @Volusiano & @Neville. My purpose is to understand how to interpret the REM results and how to adjust the hearing aid using the manufacturer’s fitting program. I have watched the video of Dr. Cliff regarding REM and he mentioned that at the initial fitting using manufacturer’s algorithm it will likely deviate from the prescriptive amplification in REM. If that is the case, the audiologist needs to adjust the amplification of the hearing aid using manufacturer’s fitting program then run the REM again to see if it matches the prescriptive target. So how does one adjust the gain on moderate, loud & soft using the manufacturer’s fitting program by referring to the deviation in the REM. As a example Phonak Brio 5 has 9 automatic programs (e.g. quiet, noise, loud noise, echo etc.). Since 3 curves should be adjusted where do you start adjusting these 3 curves in manufacturer’s fitting program. Do you have to adjust each curve in each automatic programs then run the REM again?
I’ve programmed my Phonak Hearing aids with the REUG curve given by the audiologist.
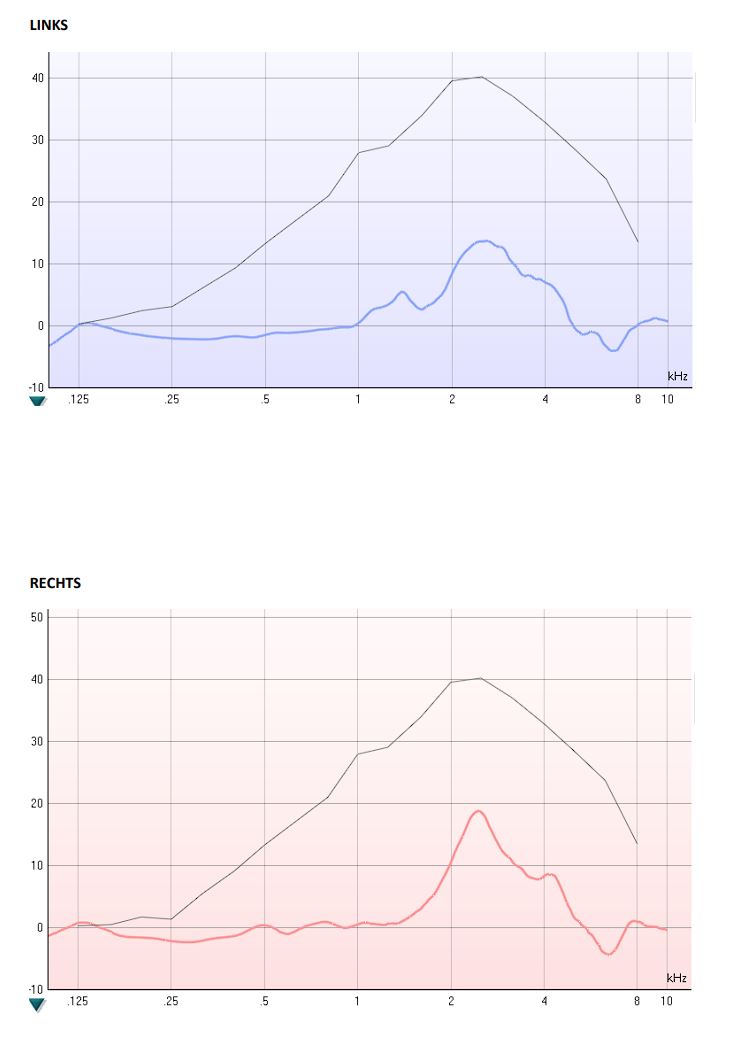
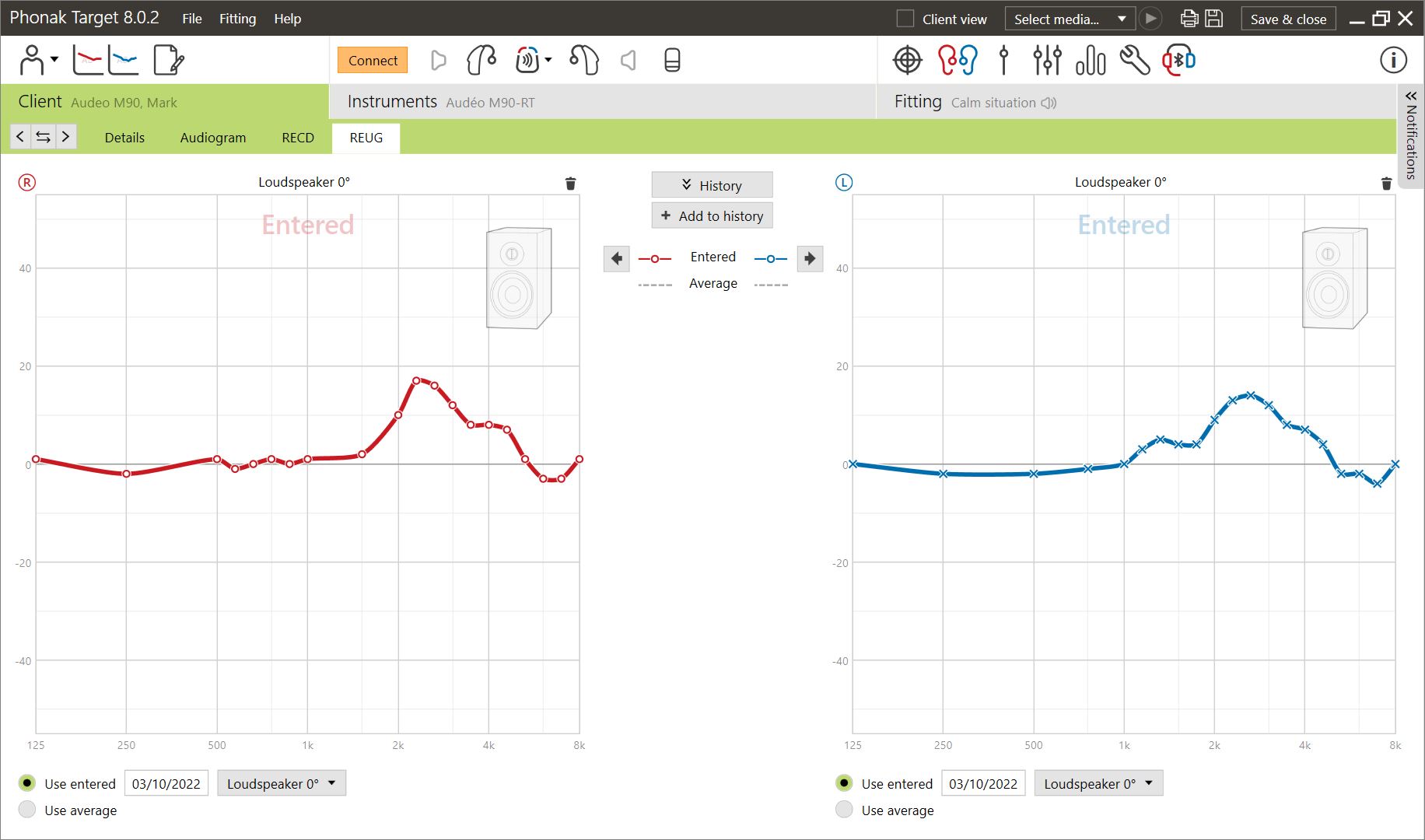
(The trouble with data input is that the frequencies available in Phonak determine the form. So if a peak is between two frequecies it results in a platform.)
Looking at the explanation on this page the REAG should also only give you one set of value-pairs: difference versus frequency. Just with the aids on inside the ear.
Phonak’s other tab for RECD also only allows one set of value-pairs. This also follows from the explanation given on the linked page.
So I don’t think that you were given REAG values. Rather I think you were given your amplification values that took into consideration your REAG values. (Apparently, DSL even needs those before the aids can be fitted.)
I remember when I trialed Audika G500’s, I hooked them up to my PC using a serial Hi-Pro. I loaded the settings from the HA’s and found the REUG values sitting pretty:
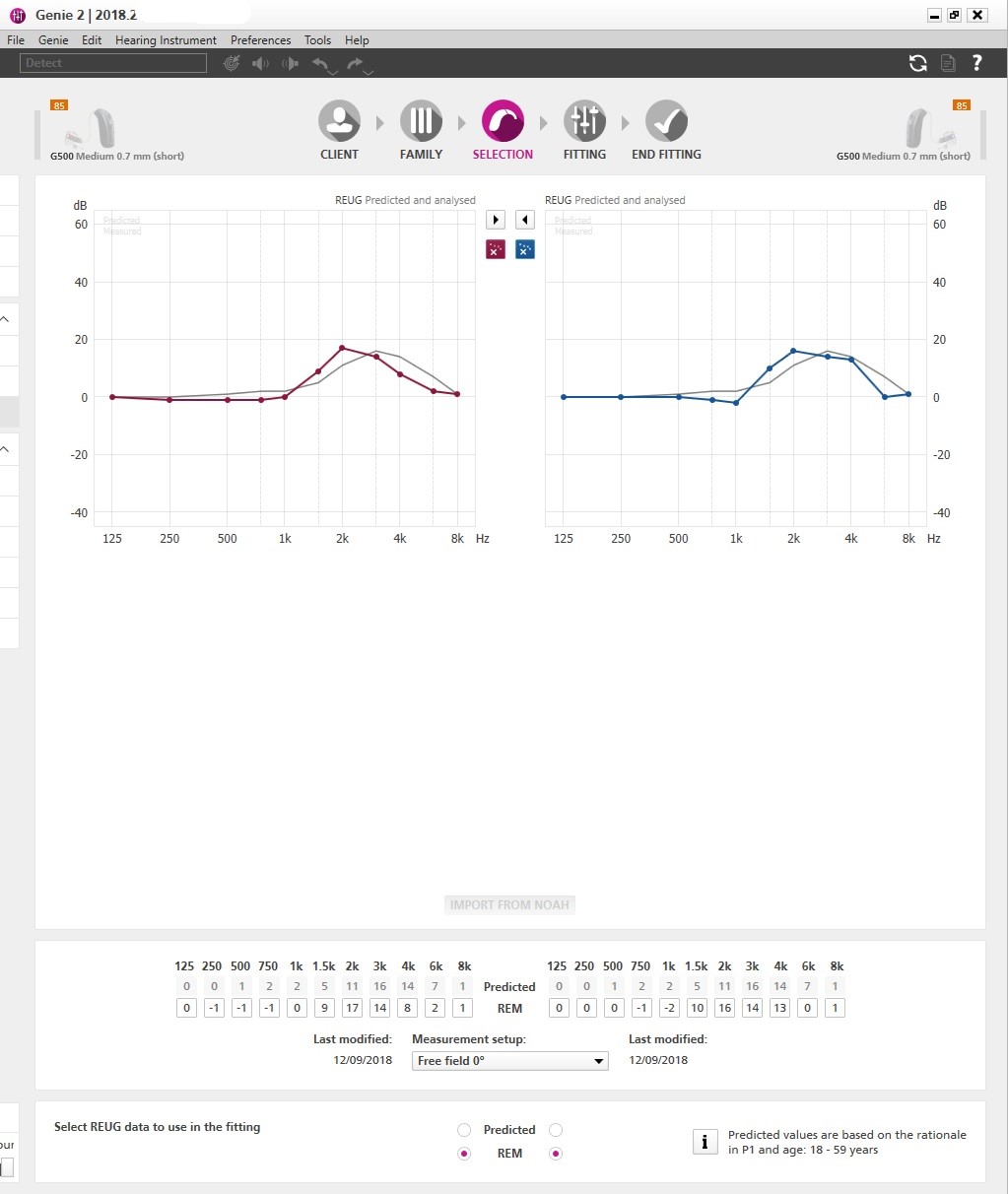
So maybe you could take another look at the software?
Gross to fine, typically. Adjust all programs together overall, typically frequency first (again, gross to fine) until you are matching the 55 dB curve, and then you check compression and sub-programs, so on.
But there isn’t a firm one-to-one relationship between the steps in the manufacturer program and the results in REM, so you’re basically just turning things up “some amount” and then running the curve again to see whether you are where you want to be or you’ve overshot. For some manufacturers, one step is bigger and for some one step is smaller and you get to know that with experience. Additionally, lack of change on REM after software adjustments will highlight other problems, like acoustic coupling issues.
Thanks for the explanation. Now I understand why I cannot see a pattern how the Costco Japanese audiologist is adjusting the Brio 5 in Phonak Target as he shifts from REM to Target to align with REM prescriptive amplification.
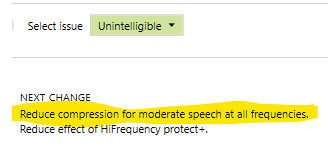
I am trying to understand how the Phonak Target automatically fine tunes the hearing aid with “unintelligible” issue. Could you please advice the steps on how to manually “reduce compression for moderate speech at all frequencies” to improve intelligibility? The Phonak Target does this automatically, but it would help if we know the steps and execute manually so we can understand the concept. Thanks.
I came across this thread when I did a search for “diy”
I’m very interesting in learning more about self adjusting my hearing aids.
DaveL
Toronto
All of my audiologists used REM until the last appointment with the audi that provided my hearing aids.
He did a quick fit using Target.
I’ve moved on.
The new practitioner did a quick fit too. I can finally hear.
I’m confused though. I don’t understand why the hearing aids didn’t work for me using REM, then were reset using a quick fit by someone else, and they work so much better.
DaveL
First of all, REM doesn’t always improve the HAs’ performance from their initial gain prescription. If the HAs perform up to snuff to begin with and don’t underperform, and/or if the fitting selection and ear canal shape are the ideal choices and ideal conditions as to not drag down the HA’s prescribed performance further, then the clinician will see that the initial prescribed gain curves already matching well against the target gain curves, and therefore no further adjustment is needed. From this point of view, you can walk into a REM session and walk out of it with the exact same result you came in with no improvement, because nothing needs to be adjusted/improved. In this case, REM does not equal “better”. In this case, REM equals “verified to be up to snuff against the target already, no further adjustment needed.”
Now it’s not clear how REM was done in your case. If it was done by an external standalone REM setup, then most likely REM will be performed against a standard fitting rationale, probably NAL-NL2. This is because the mfg’s proprietary fitting rationales is private (a trade secret) and the external REM machine can only work with standard/publicly know rationales.
If the mfg’s programming software (in this case, Phonak Target for you as a Phonak user) can accommodate and support a number of REM equipments, and allow its Target software to work well with these REM equipments, then the Phonak APD proprietary fitting rationales can be calculated by the software target to be APD-based, because this Target software has the knowledge to calculate using APD rationales, while the external REM software doesn’t.
So let’s say you had REM done with an external/stand-alone REM hardware/software setup, then most likely it’s set to the standard rationale NAL-NL2 as the target. Even if the original prescription was the Phonak proprietary-based APD rationale, the clinician has now adjusted to “force fit” it into the target NAL-NL2 standard already.
The standard rationales may not work wonder for everybody. Some who have always used it and are used to its characteristics may prefer it to mfg proprietary rationales. Apparently for you, your ears don’t like the standard rationales for certain reasons. It seems like your ears like the Phonak APD rationale better. So that can explain why you found the REM adjusted result (to NAL-NL2) not as good as the proprietary APD rationale that was most likely used in the “quick fit”.
Even let’s say that you have “virgin ears” and have not been exposed to either rationales, so they couldn’t possibly have a preconceived notion to favor one over the other, remember that standard rationales don’t know much about the hearing aids per se, and therefore a lot of assumptions had to be made about how the hearing aids work in order for the developers to arrive at a more “universal” rationales that got adopted as standard.
On the other hand, the HA mfg who developed their own proprietary rationale specifically made for their own HA brand has intimate knowledge of how their own HAs work, and therefore no assumptions had to be made about how their HAs work (unlike the assumptions that had to be made in the development of the standard rationales). So it’s possible that the HA mfg’s proprietary rationales used in the “quick fit” simply just work better for their brand of HAs compared to the standard rationale that might have been forced fit to your HAs when REM was done. And the proprietary rationale may work better because they fit their own HA’s brand better like a glove.
2 Likes
REM is not about doing anything in and of itself. It is simply about measurement of the sound that is being produced at (or close to) the eardrum by the HA.
It is intended to provide the audiologist with absolute feedback as to how well or otherwise the prescription is being delivered by the HA setup, taking account of HA build and ear canal geometry.
Accordingly, REM doesn’t care whether a proprietary algorithm was used to program the HAs or if it was done using a NAL/NAL2 protocol.
If everything is good with the HA fitting, regardless of the protocol used, it will give the audiologist REM information that helps him/her to know that the sound at the eardrum is as intended. It will also show if the HA is not performing as intended and/or if the ear-canal is so geometrically different from an average that it is affecting the sound being heard, allowing the audi. to adjust the program to accommodate the differences or to consider that a device may be faulty.
Of course REM isn’t a person so REM doesn’t care about anything. REM is simply a method (considered best practice) to verify how well the HAs, the fitting, and the whole system perform. To verify this, there has to be measurements (hence the mics placed inside your ear canals), and the reference which is to be measured against. The reference is the yard stick, or the target, that tells the clinician whether the whole system performs to target or not.
REM may not care which fitting rationale the target is based on, but the clinician should care to pick out the proper fitting rationale that’s available in the REM equipment which is appropriate for the patient. For example, the clinician shouldn’t pick the DSL Pediatric rationale designed for children and use it as a target gain curve for adults, and vice versa. In this sense, the choice of the target gain curve is very relevant.
Ideally, if the clinician can only generate an NAL-NL2 based target gain curve on his/her REM equipment, then the clinician should have selected the same NAL-NL2 in the HAs’ program so that they match and perform accordingly. Otherwise, let’s say if the clinician choses the Phonak ADP rationale as the default initial prescription for the main program in the Phonak aids, but then does REM using the target gain curve calculated based on NAL-NL2 and adjust the prescribed ADP gain curve to the NAL-NL2 target gain curve, the end result will sound like you’re hearing an NAL-NL2 based program at that fixed volume. But as soon as the volume dynamic changes, the volume fluctuations will behave in accordance to what the ADP rationale dictates, and will NOT behave in accordance to what the NAL-NL2 rationale dictates.
So unlike what you said, the choice of the proper fitting rationale to be used to calculate the target gain curve in REM to make adjustment to is not irrelevant. One shouldn’t use a target gain curve based on DSL Pediatric to do REM on adult for sure. And if one can only do REM with a target gain curve based on NAL-NL2, for example, then one should select NAL-NL2 as the rationale of choice in the HAs’ program as well, so that they’re better matched and well matched. Otherwise, it can lead to confusion like @DaveL has shared, as to why his REM adjusted result doesn’t sound as good as his “quick fit” result → most likely because they don’t match in the first place, and @DaveL has his own preference of one over the other.
If ADP is chosen as the prescription for the HAs’ program, then if during REM, it’s compared against an NAL-NL2 based target gain curve, most likely it’ll seem like the HAs “underperform” against the target curve, especially in the highs (because NL2 puts aggressive emphasis on the highs for speech, but ADP may not be as aggressive on the highs for speech. So that may simply be because the ADP rationale doesn’t put as much focus on the highs as NAL-NL2 for speech priority, not because the Phonak HAs underperform and don’t match the target. If the target gain curve had also been ADP based, then the likelihood of the ADP-based prescribed gain curve matches better to the ADP-based target gain curve would probably increase.
My old audiologist quit. He referred me to a list of others. He had tried for two years. We parted friendly.
He never use NAL-NL2. I watched the screen as he worked. I’m not his client anymore, but am using a wonderful company named “Hearing Well Matters”
The last setup with the old audiologist he informed me that my hearing aids would be quieter because my hearing had improved. In fact the audiogram he used is about 10 dB less than previous audiograms he and others had provided. So my hearing was worse from him and the previous audiologist.
I called into Hearing Well Matters yesterday. I requested a new hearing test and setup. That will happen in a week or so…
Have to run. I’ll be back.
DaveL
Toronto