To expand on @tenkan 's point, my understanding is that if a REM stand-alone system/equipment is used, then it’s natural to understand that this REM stand-alone equipment can only have access to the standard fitting rationales, hence without access to the proprietary fitting rationale of a HA mfg, it cannot perform REM against a proprietary target curve because it wouldn’t know how to generate one.
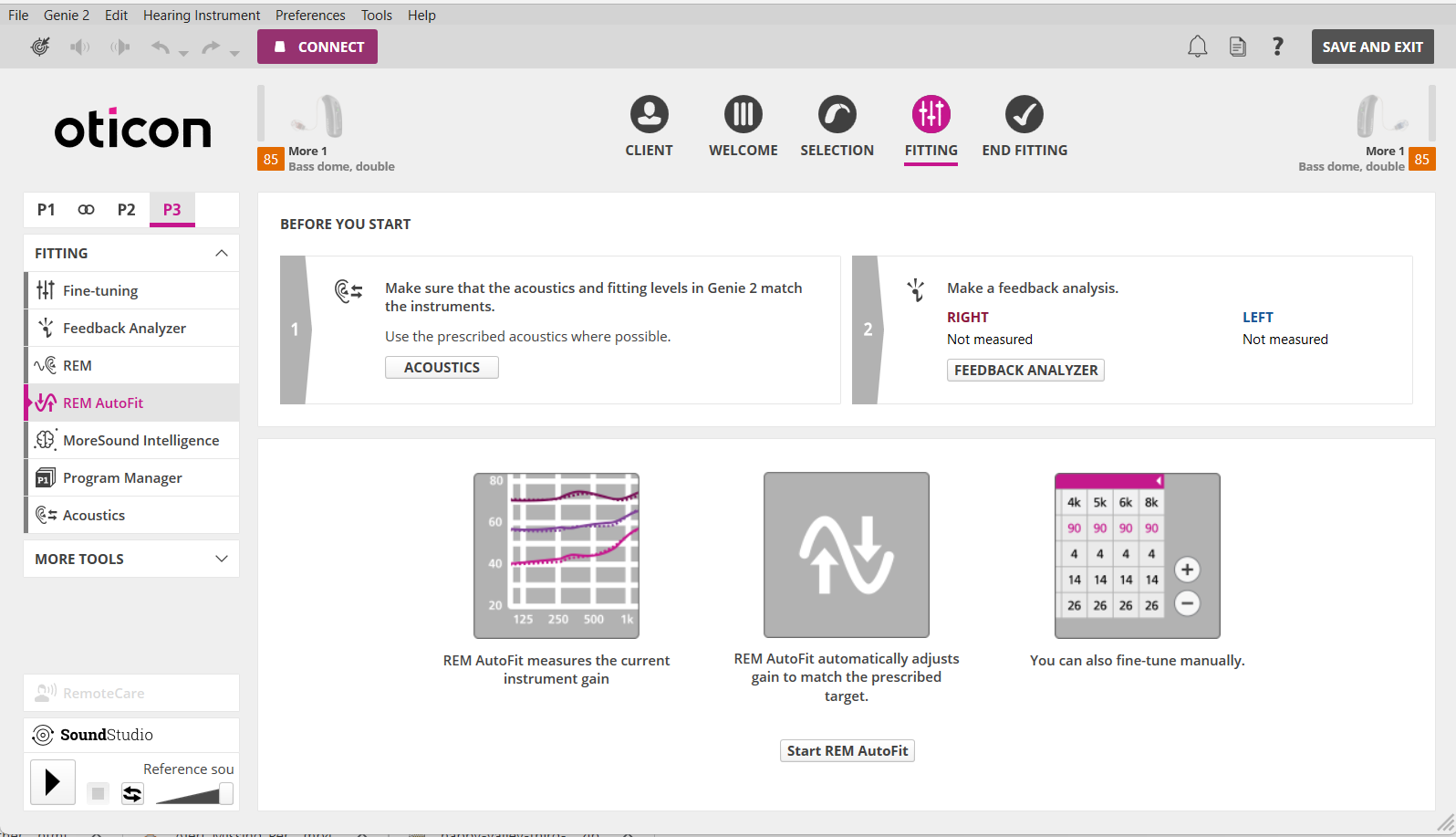
But I notice that the Oticon Genie 2 software as something called REM Autofit (see screenshot below). I assume that as long as the HCP has REM equipment that is compatible with the Oticon REM Autofit, then REM Autofit can deliver the proprietary rationale’s target gain curve to the REM equipment so that adjustment can be done against the proprietary target curve. This would solve the issue of a stand-alone REM system that can only be fitted against a open standard fitting rationale.
This is just my assumption because it seems to make sense, but I don’t know enough about REM equipment to know if this assumption is true or not.