Hi Samyak,
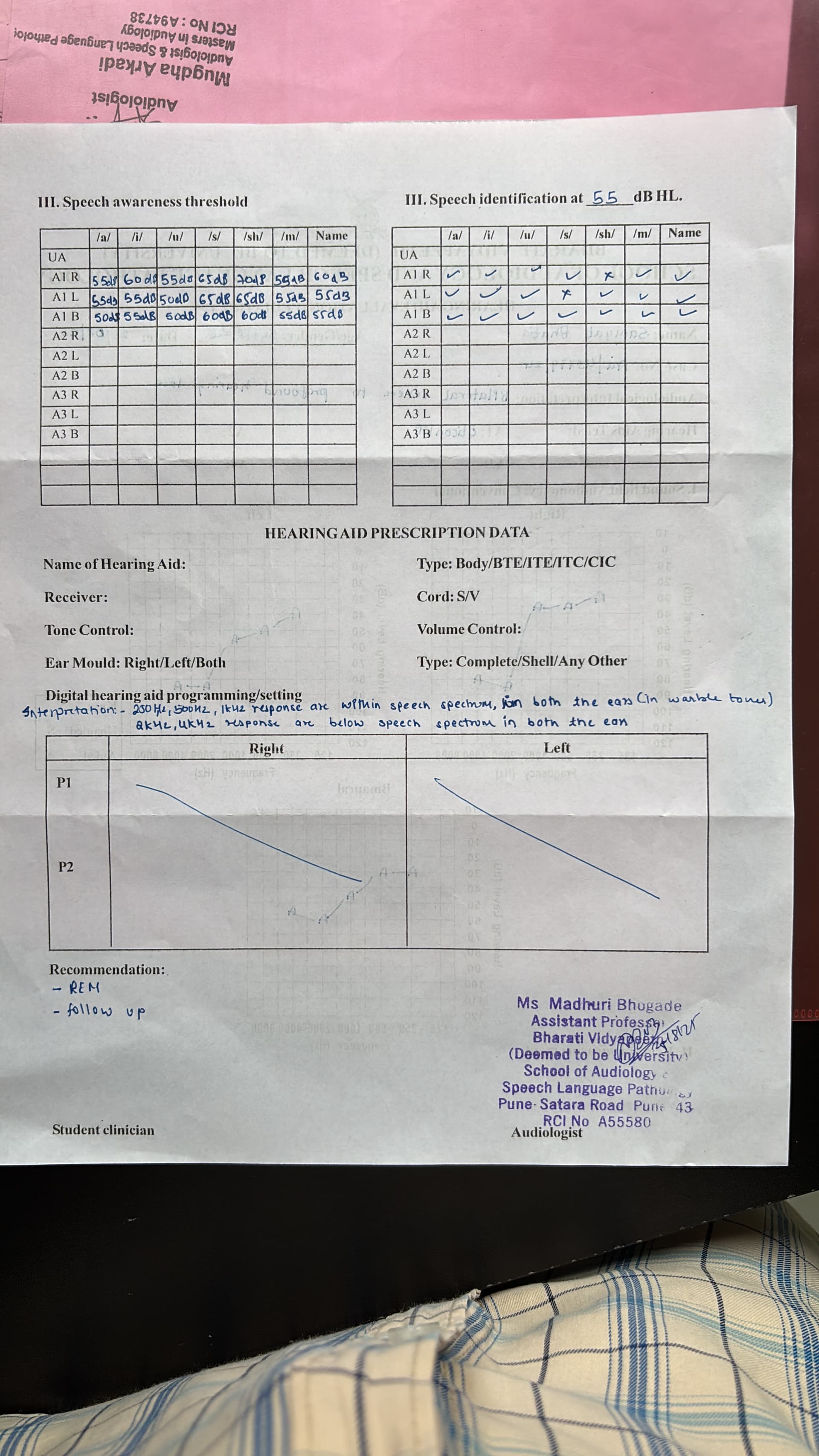
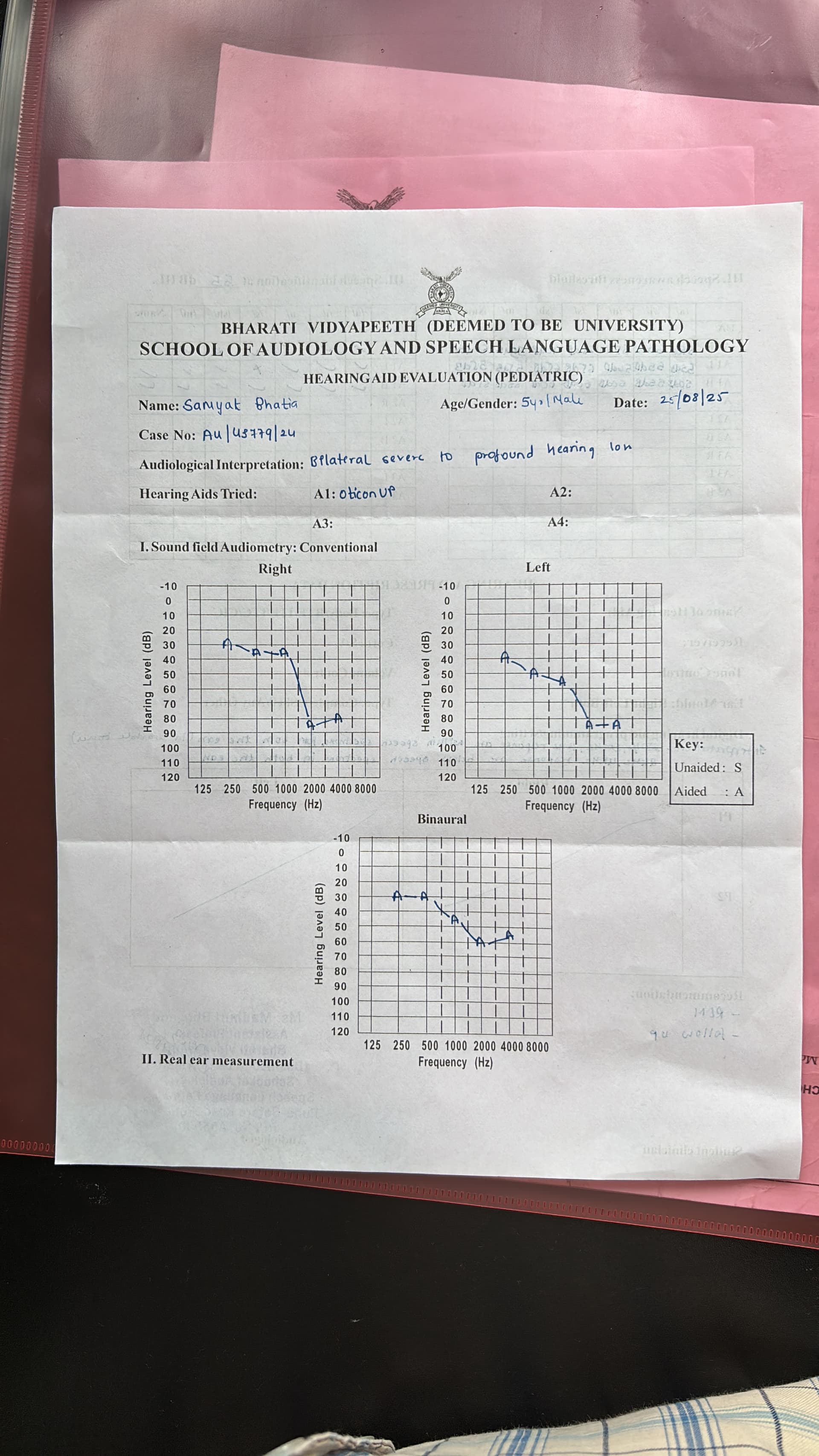
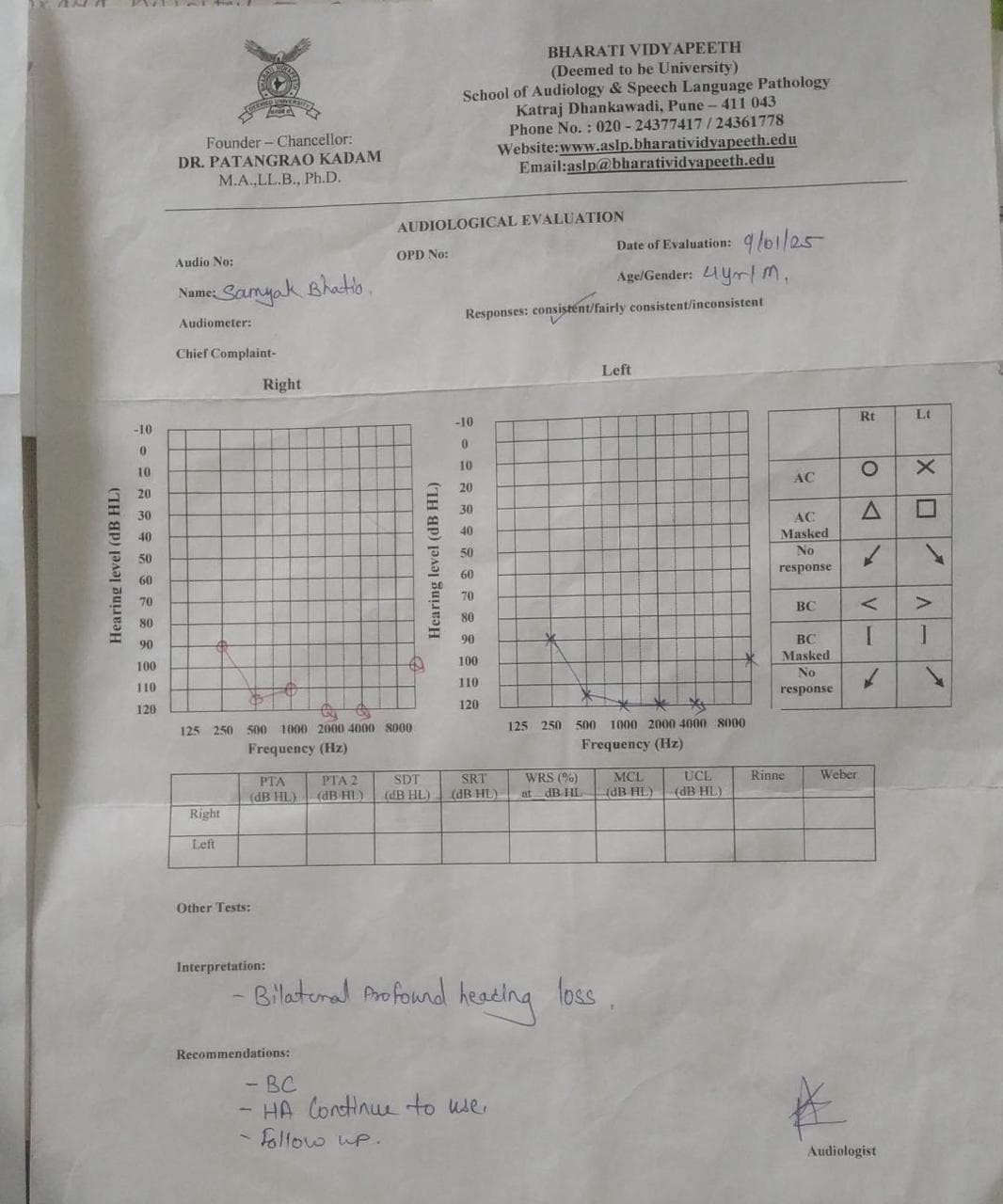
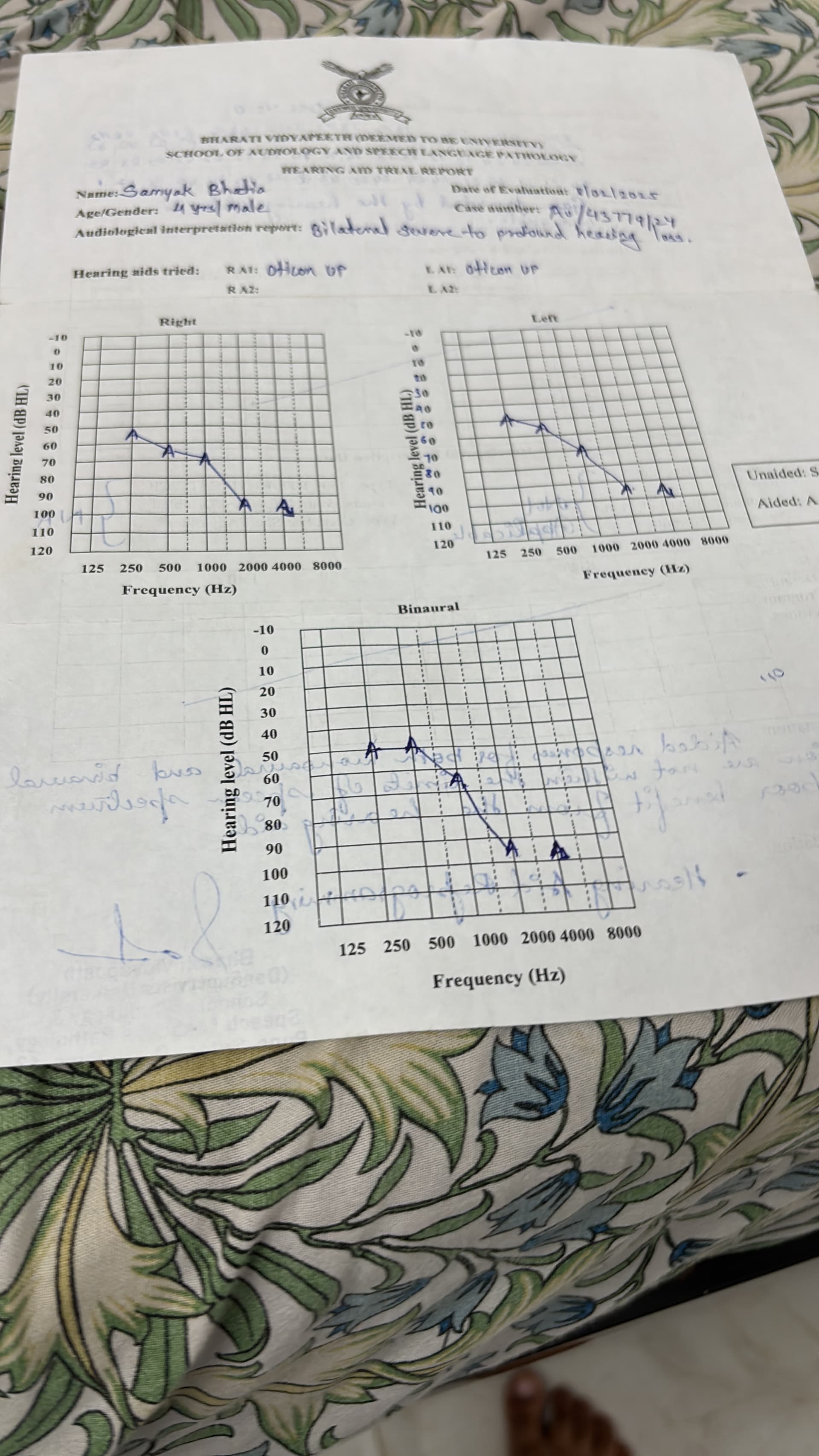
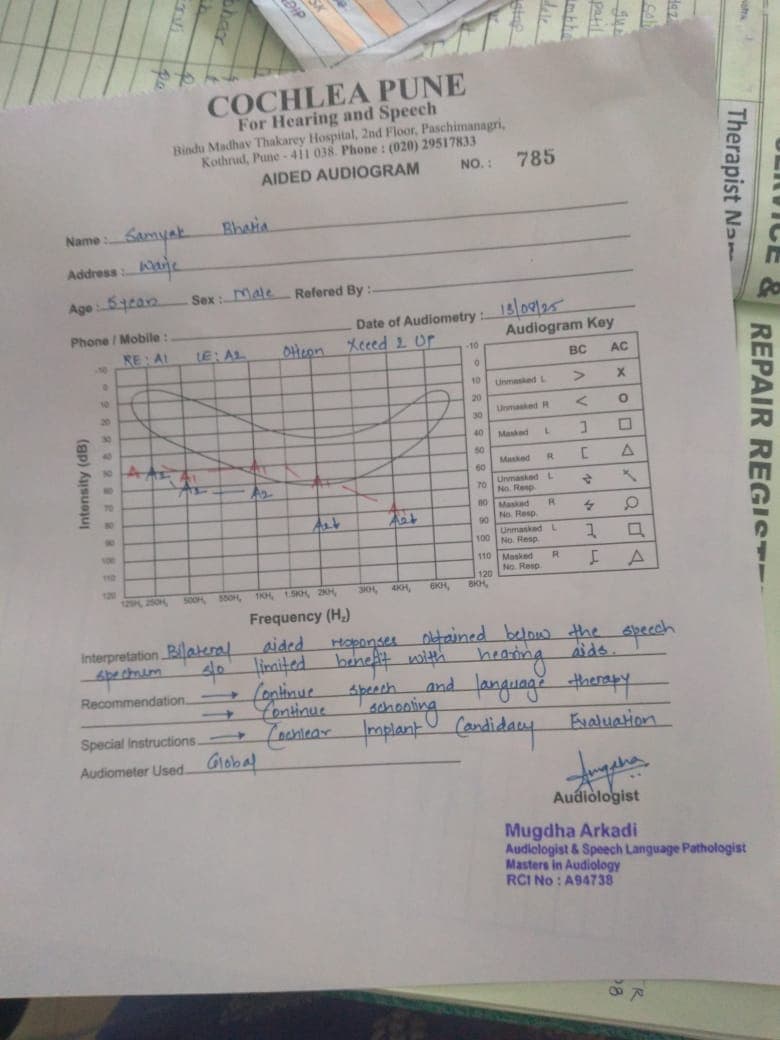
Unfortunately it seems that you are misunderstanding the aided audiogram results. None of the aided responses fall into the slightly elevated category, even in the low frequencies. The aided audiogram shows a mild sloping to moderate elevation in hearing thresholds. This is much worse than a “slight elevation.”
The speech intelligibility index (SII) is a better predictor of the audibility of speech sounds. It ranges from 0 for no speech intelligibility to 100 for perfect speech intelligibility for someone with normal hearing. A child needs an SII score of at least 80 for average level speech in order to develop speech and language normally.
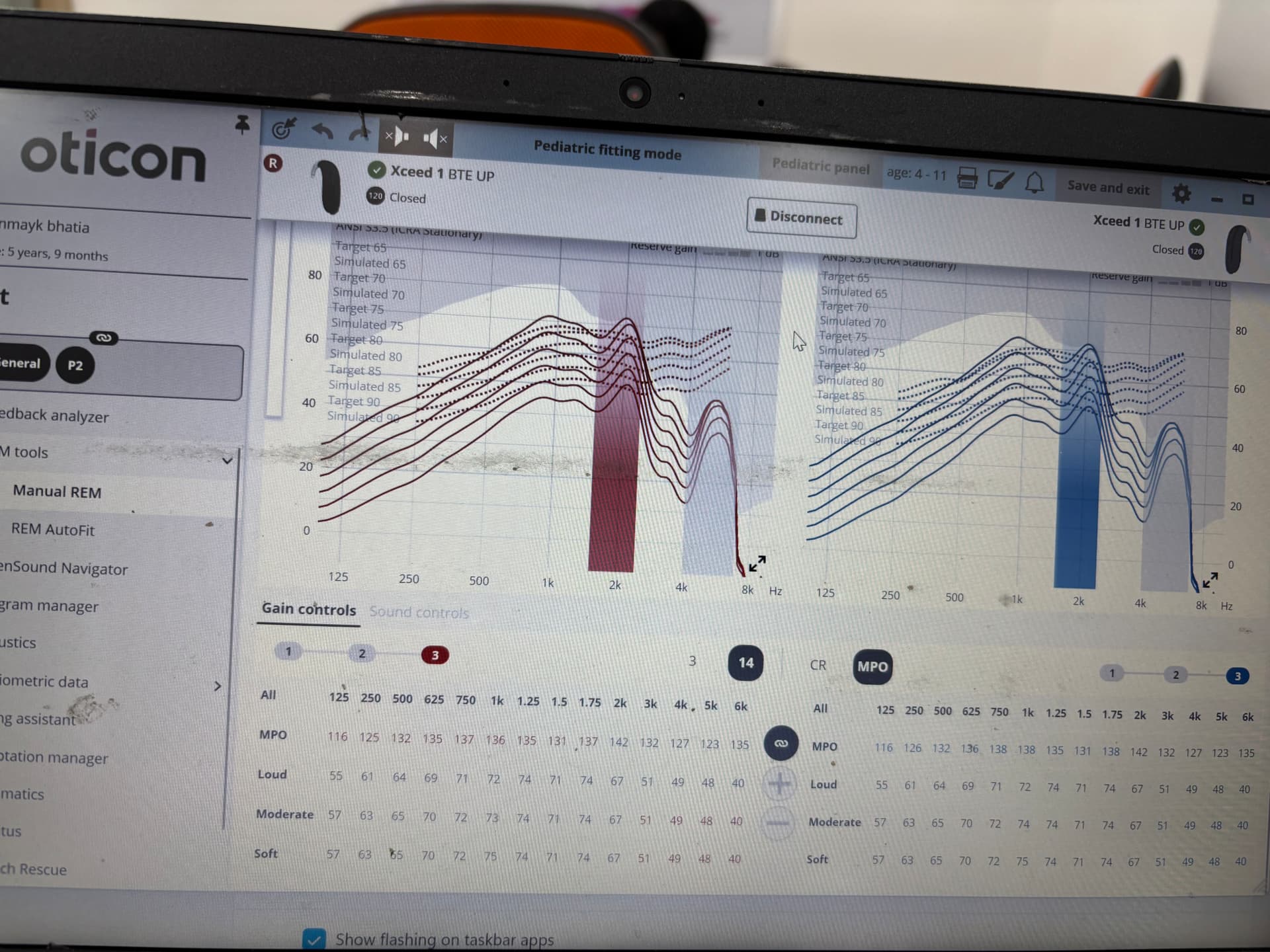
Without his hearing aids your child has an SII of zero as he is unable to perceive sound at all. Based upon the aided thresholds you have provided the best case scenario is that with hearing aids he could have a SII of 10 for soft speech, a SII of 27 for average level speech and a SII of 54 for loud speech.
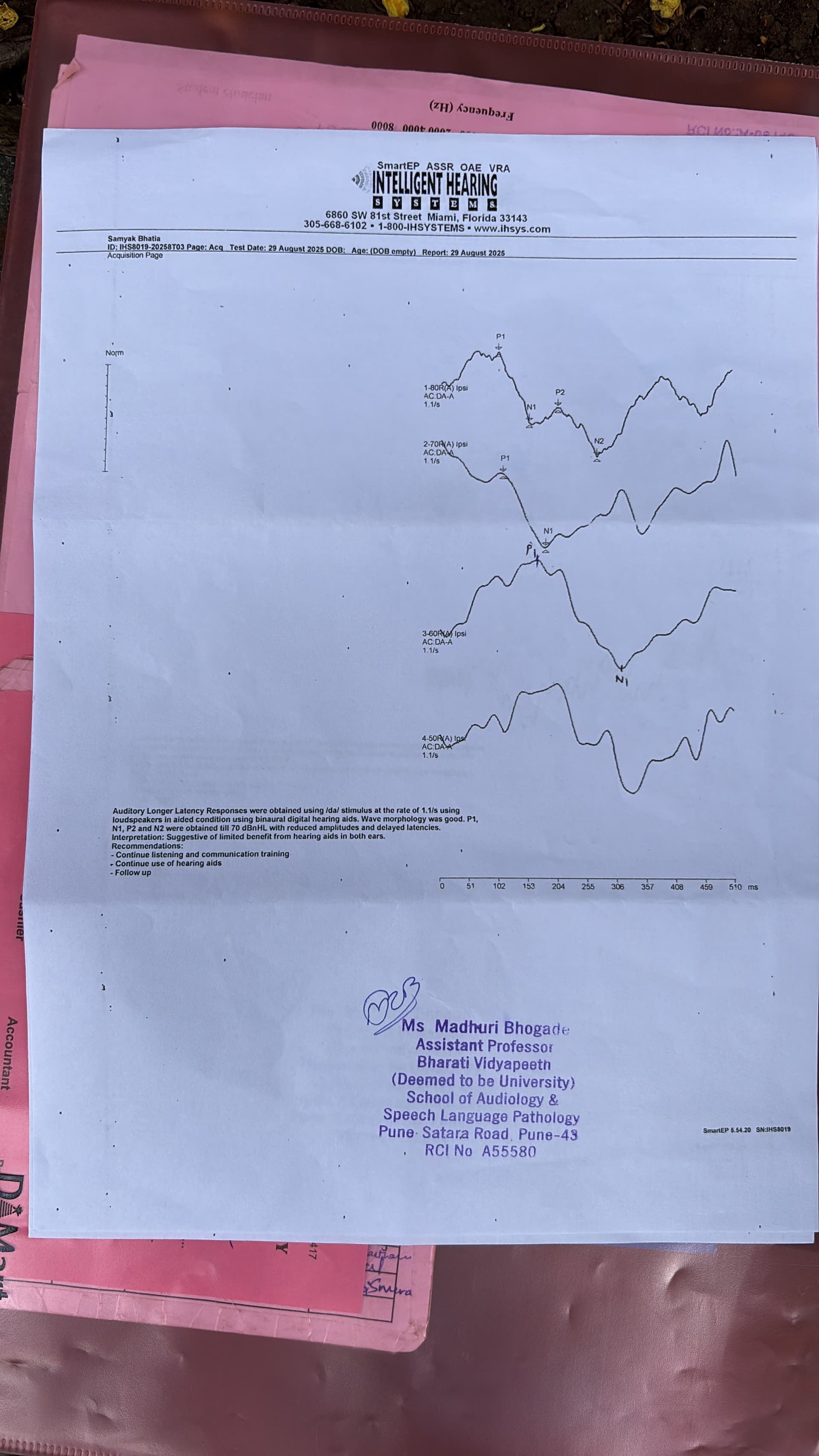
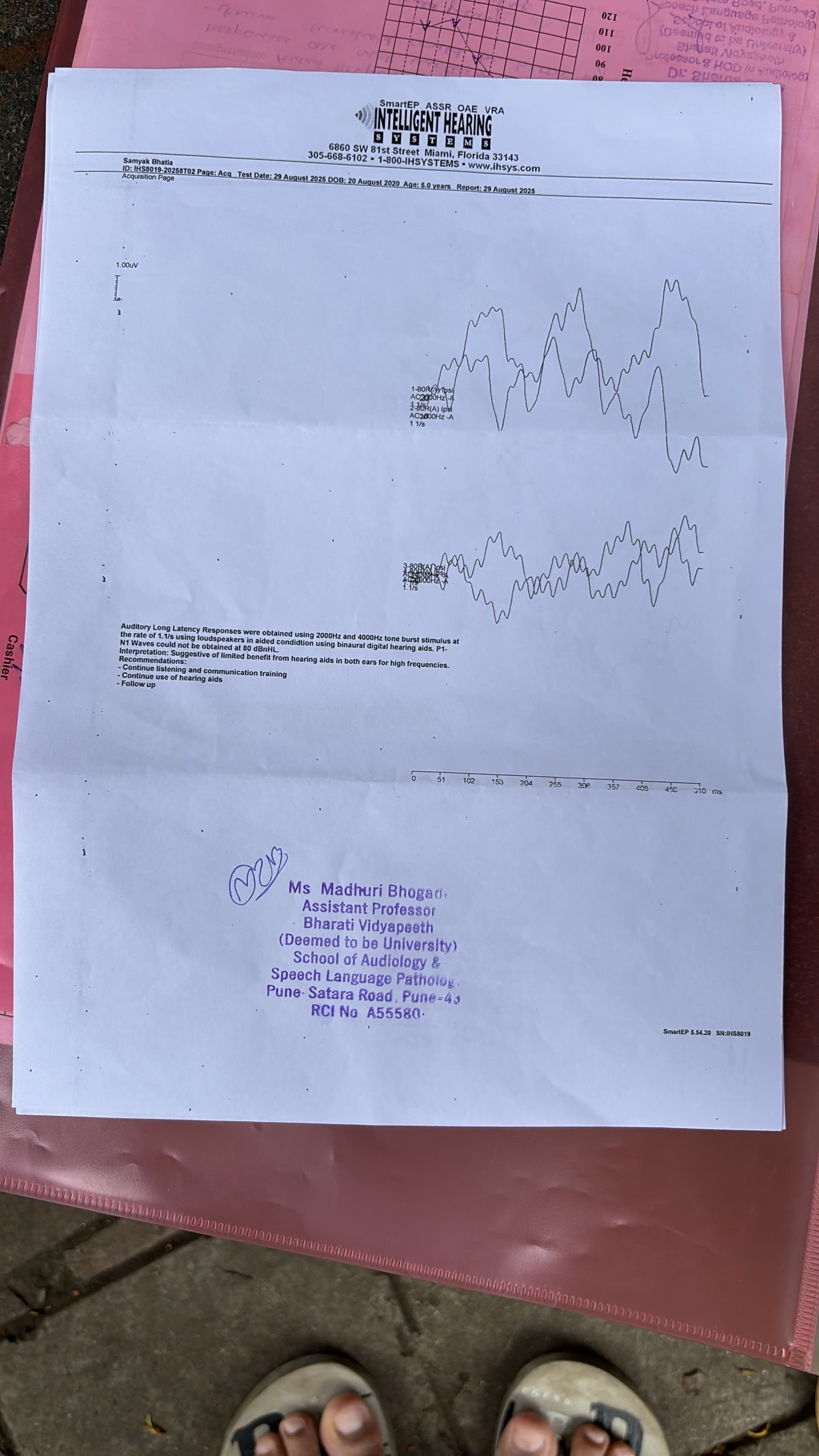
All of these values are well below 80 indicating that even with optimally fit hearing aids your child won’t be getting sufficient audibility of speech for speech and language development, even if people are talking very loudly directly into their hearing aids all day, every day.
Hearing aids couldn’t have ever provided your child with sufficient audibility of speech for normal speech and language development. There simply isn’t enough residual cochlear function for this. As a consequence of his inability to hear most of the speech sounds consistently he will also struggle with reading and writing, because hearing sounds consistently is a pre-requisite to associating them with visual symbols. You cannot attach meaning to something that is out of your perception.
A cochlear implant typically results in aided thresholds of between 15 and 30dBHL across the entire speech frequency range which will provide your child with much better audibility of speech which is necessary for continued speech and language development.
While surgery is involved with cochlear implantation, it is one of the safest and simplest surgical procedures an otologist performs with very low rates of complication. There are more than 650,000 cochlear implant users worldwide and the rates of implant failure are also very low, with many users still using the same implanted components they received back in the 1980s.
I would very strongly recommend that you reconsider cochlear implantation if you want your child’s speech, language and cognition to continue developing. The benefits strongly outweigh the risks and have done since your child was first diagnosed at 22 months of age. Every month you delay this the predicted long-term outcomes for your child’s speech and language development and cognition (even with a CI) only get worse.
In saying this, if you would prefer that your child live in the Deaf community and be in full immersion sign language there is nothing wrong with continuing the way that you are. Your child’s hearing aids provide them with enough environmental awareness of sound to be safe in most environments. They just don’t provide sufficient hearing for good speech and language development. In the long term they’ll likely need to rely on sign language for communication as hearing loss worsens as you age and choosing for your child to live in the Deaf community with full sign immersion is a legitimate choice. However you’ll also need to be fully involved with the Deaf community as well.
Whatever your choice I know you’ll pick the right one for you and your family. However if you don’t want full immersion sign language for your child in the long term then your only choice is cochlear implantation and you need to be making that decision in the very near future. Your child may no longer be considered a candidate for implantation in a years’ time.