I appreciate all the feedback. Trying hard to learn from others as much as possible. Regarding your question- no conductive loss. Thanks.
3 Likes
The point is that citing statistics for the general population is kinda irrelevant when you’ve arrived at a posteriori condition:
What is posterior probability?
Posterior probability is the revised probability of an event occurring after taking into consideration new information .
What Does a Posterior Probability Tell You?
Bayes’ theorem can be used in many applications, such as medicine, finance, and economics. In finance, Bayes’ theorem can be used to update a previous belief once new information is obtained. Prior probability represents what is originally believed before new evidence is introduced, and posterior probability takes this new information into account.
I used to consider Bayesian probability all a bunch of hogwash and happened to work down the hall from a guy who lived and breathed by it (and eventually won a Nobel Prize - and modestly disclaimed in making his Nobel Prize-worthy advance that he had any inkling that his work would blossom into an idea of that caliber!).
The reason at the time that I dredged up to dispute the value of Bayesian considerations is that you rarely if ever have good enough data on how the posteriori condition, e.g., a patient is diagnosed with FLAT sensorineural hearing loss, affects the posteriori probability, what are the chances that this loss is caused by heart disease (or the reverse Bayesian probability, if a person is diagnosed with some sort of cardiovascular disease, what are the chances that they will suffer hearing loss?).
However, I’ve had to get some new religion. Bayesian probability is highly used in machine learning, e.g., what are the chances in speech recognition that a person said the syllable “er” or the word “dog” - the chances that either the syllable or the word was uttered depend conditionally on what was uttered around it in a Bayesian way and the whole probability is chained together to get an extremely difficult probability calculation (requiring a powerful computer) that a whole phrase was uttered in a particular way, e.g, “dogs love cats” vs. “dogs hate cats.”
So in the same way as speech context, the knowledge that Johnmurphy has very flat, non-conductive, probably sensorineural hearing loss changes the probabilities as to what underlying causes might be relevant, just in the same way that very rapid unilateral hearing loss in just one ear drastically changes the probabilities of what might be likely in the affected individual. It’s just in Johnmurphy’s case, we really have no good idea what the relevant Bayesian probabilities might be for any potentially contributing condition like cardiovascular disease. Could be the same as the a priori general population probability, might not be - but to assert that the probability is the same as before knowing John’s condition is not right, even though it’s entirely possible it’s the correct answer.
BTW, John, there is a slight ambiguity in your answer. I interpreted your answer to mean that you do have a conductive loss of hearing that’s ~identical to your through-the-air loss, indicative that you’re loss is entirely sensorineural. Interesting that audiologists/ENT folks, etc., have never ironed out the ambiguous terminology surrounding the phrase “no conductive loss.” Perhaps all depends on charted data, boxes checked, blanks filled in, and less worry about flinging words alone around.
Heh. What’s ambiguous about no conductive loss? If your bone conduction scores are identical to your air conduction scores, you do not have a conductive loss.
Or if this helps disambiguate things for you–if your air line is at 60 and your bone line is at 40, your conductive loss is 20, not 40.
3 Likes
Edit_Update: Perhaps the distinction is in the use of the two terms “conduction” vs. “conductive” and “CONDUCTIVE” is only used as an adjective in describing the category status whereas CONDUCTION is used to describe a test of “conductive” status - again, a better choice of terms would have helped. But once one learns something in school, it becomes the gospel…
Audiologists might take for granted language naïve members of the general public misconstrue, i.e., “no conductive loss” means you DO have bone conductive loss, not “no bone conductive” loss but the categorization means the loss you do have is not categorized as “conductive loss” - so audiologists, in one phrase, manage to confusingly refer (from the general public standpoint) to apples and oranges at the same time - they could have picked a somewhat different name for the category or the terminology for status in the category vs. the actual loss measurement. You have a bone conductive loss means no conductive loss, get it?! ![]()
P.S. Sometimes problems in nomenclature arise when names and terms are picked before the underlying bases of the phenomena are fully understood - don’t know if that applies here to tests vs. categories and upstream/downstream flow in hearing but “positive” and “negative” in batteries and which way electricity actually flows would be an example of where they decided on concepts before they understood the underlying basis fully… Which Way Does Electricity Flow?
No it doesn’t. It means you have NO conductive loss.
1 Like
I’m baffled by this confusion. But maybe you’re right and I am taking something for granted. Are you thinking of it like. . . “his thresholds via bone conduction are normal, so he has no hearing loss when tested via bone conduction, indicating that his air conduction thresholds are due to a conductive loss”? That IS super confusing. But no one says that.
(edit: I read it again and it did not confuse me. But if I twist my brain around enough I think I can see the issue.)
1 Like
As I noted above in a correction as you were typing, I should have said in the two lines above: Moderate loss diagnosis - #29 by jim_lewis
No CONDUCTIVE loss (in the category status) means you do have a bone CONDUCTION loss (test result) that matches your over-the -air measured loss, i.e. your loss is sensorineural, not CONDUCTIVE status type.
and
You have a bone CONDUCTION loss (test result) that matches your over-the-air loss means that you have NO CONDUCTIVE loss (category status), rather a sensironeural loss.
I could be very wrong - apologies if I am and for being a smartie pants, but I think the distinctions rely on the usage of modifying terms in a base word to tell the listener whether one is referring to a type of hearing test or a category status for a type of hearing loss as determined by that hearing test relative to an over-the-air hearing test.
No, but that would never be said. You would never refer to the bone score as a “bone conduction loss”. Cuz you’re right, that’s very confusing. The conductive loss is the gap between that and the air threshold. People will say “bone line” or “bone scores” but not “bone loss”.
It’s late at night and now the word conduction AND the word bone have lost all meaning through repetition.
I do like semantics though. ![]()
My comments are not worth staying up for! Enjoy a well-earned night’s rest!
The paradox would be, though, that both over-the-air results and bone conduction tests can be graphed on the same chart (chart shows identical OTA and bone conduction results ~superimposed, purloined from https://www.osha.gov/dts/osta/otm/new_noise/#hearingloss):
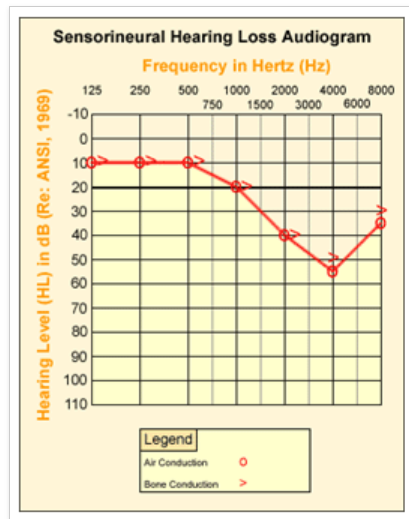
So lots of people on the forum refer to the depiction of over-the-air results as showing HEARING LOSS but the irony in audiology is that we will not refer to the bone conduction results as showing a BONE CONDUCTION LOSS but just rather low bone scores (whatever that means! ![]() ). I would suggest that the different semantics was necessary to keep things straight between bone conduction tests and conductive category status. Maybe clearer semantics is not necessary for well-trained audiologists but for naïve members of the general public, it might be easier to understand what a bone conduction loss means rather than low bone scores. In plain English, the graph above clearly shows both air conduction loss and bone conduction loss compared to normal hearing (although the further irony is that when you see bone conduction results matching over-the-air conduction actual bone conduction is probably normal, i.e., no loss, because the defect is sensorineural (in the inner ear or beyond) - so perhaps it’s the paradoxical nature of the test results that generates the terminology conflicts - like electricity actually flowing in reverse to the classical assumed current path out of a battery-bone conduction is an artificial alternative test-and it’s really a test of the function of the air conduction pathway-an absolutely normal bone conduction test vs. the air conduction test means that you DO have a problem in the air conduction pathway in the outer or middle ear, in my ignorant grasp of the subject).
). I would suggest that the different semantics was necessary to keep things straight between bone conduction tests and conductive category status. Maybe clearer semantics is not necessary for well-trained audiologists but for naïve members of the general public, it might be easier to understand what a bone conduction loss means rather than low bone scores. In plain English, the graph above clearly shows both air conduction loss and bone conduction loss compared to normal hearing (although the further irony is that when you see bone conduction results matching over-the-air conduction actual bone conduction is probably normal, i.e., no loss, because the defect is sensorineural (in the inner ear or beyond) - so perhaps it’s the paradoxical nature of the test results that generates the terminology conflicts - like electricity actually flowing in reverse to the classical assumed current path out of a battery-bone conduction is an artificial alternative test-and it’s really a test of the function of the air conduction pathway-an absolutely normal bone conduction test vs. the air conduction test means that you DO have a problem in the air conduction pathway in the outer or middle ear, in my ignorant grasp of the subject).
I think the main thing that makes “bone conduction loss” sound so wrong, is that it implies some abnormality of the skull.
3 Likes
I take @Johnmurphy 's “no conductive loss” statement to mean that there is no loss present that is determined to be of a conductive nature. I suspect that’s what he intended. But, you know what happens when one assumes.
Correct. Sorry for not explaining better but totally new to this.
2 Likes
I think if one is going to use both the terms “air conduction” and “bone conduction,” - see the OSHA figure above for usage example, it would make the most sense to help naïve members of the general public understand to always describe conductive loss as “air conductive loss.”
And the tie-in would be straightforward: “The deficit observed in your air conduction pathway hearing test along with the normal response in the bone conduction pathway test shows you have an air conductive loss somewhere in that pathway to the inner ear.” Or: "The equal response deficits observed in both the bone conduction and the air conduction pathway tests imply that your hearing loss is not in the air conductive pathway to the inner ear but is a shared deficit further downstream from the point that both these two independent pathways merge in your body, somewhere in the nervous system and we call that sensorineural loss. "
One could say that using “air conductive loss” is misleading because it’s more to do with things other than air - but then why have the term “air conduction” in the first place? But getting “air” to be used as a modifier to make clear the pathway involved with conductive loss is probably about as likely as getting engineers to admit that electricity really doesn’t come out of the positive terminal of a battery and current arrows on circuits should be drawn in the opposite direction. Established habits are hard to change.
Or we could just call it Air-Bone Gap.
BC loss is acceptable imho, as you measure it from zero dB HL. And it exists as a standalone measurement outside of the AC audiogram.
It’s not worth getting a thread derailed over this as it’s certainly not helping the OP to get the right hearing aids.
6 Likes
Do you want to stay with the in the ear type hearing aids?
Do you want your aids to have Bluetooth streaming capabilities?
Do you have a Costco anywhere near you? They can save you a bunch of money and have great service with great hearing aids.
Let me tell you of my experience. I went into toe USAF in January, 1951, at the age of 17. I worked on B-36 aircraft. At that time hearing damage from aircraft noise was either unknown or ignored. I had a break in service from late 1954 to late 1955, when I reeinlisted into my same outfit. They did two things: gave me earplugs and a hearing test, when they told me I had some hearing loss. I didn’t notice it, so forgot about it, but did use the ear plugs. As time went by, I found I was playing music on my car radio a little loud because it “sounded better.” I didn’t realize I was cranking it up to hear the high frequencies. It was much later, early nineties, before I decided I needed amplification. I am now almost 87, and my loss is considerably worse, but the aids (now furnished by the VA) help a lot. I use bte aids because, theoretically at least, they offer higher high frequency gain without feedback, due, I suppose, to the greater distance between output and input. So, my experience has been that although the cause stopped a long time ago, my hearing continued to deteriorate. The good news is, I can hear well enough with aids to function.
2 Likes
John, I’m 81. I just got new ITE HA’s, which are far ahead of the ones I had for almost 7 years. These are controlled with a cell phone app, which gives me vast control over what I hear. My loss is on the severe side, so the speech enhancement is a great feature. As you age, your options will keep improving as new tech comes along. Hang in there.
2 Likes
John,
My loss is not flat, but it is progressive and genetic. During one 8 year period between my 20s and 30s I lost almost 60dB on a pure tone audiogram at one frequency. Now that frequency has been stable for decades. I’m losing hearing at many other frequencies, though.
I am also starting to use HAs full time, since even at home with my husband I say “what?” way too often. It’s a little spooky for me to think I will depend on HAs to hear people, however, a belt-and-suspenders approach is possible. Speech to text apps, backup hearing aids–and the realization than many people in the world depend on assistive devices that work really well.
I don’t know if what I am saying is helpful–others seem to have many aspects of your question already covered. I mentioned what I did because my attitude seems the key factor that affects how non-anxious and secure I am about being partially deaf with some ongoing progression at most frequencies. Being in touch with hard of hearing and Deaf folks has been a big source of comfort to me. The people on this forum are great in that regard. Be well and keep letting folks know how you are doing and how we can support you!